Why does health care cost more in some areas of the country than others? It’s a question researchers have struggled with for decades, because the potential answers — unnecessary surgeries, generally bad health of patients or high prices charged by providers — each carry different prescriptions for how to hold down medical costs.
Now a new study from the Center for Studying Health System Change takes a novel approach by comparing claims among 218,000 autoworkers in 19 metropolitan areas. Because the autoworkers had the same private health plan through their union, the study didn’t have to worry about how different insurance benefits influenced health spending.
The study found a wide variance in the health spending per autoworker in 2009, from $4,500 in Buffalo, N.Y., to $9,000 in Lake County, Ill. (The full list is at the bottom of this post.)
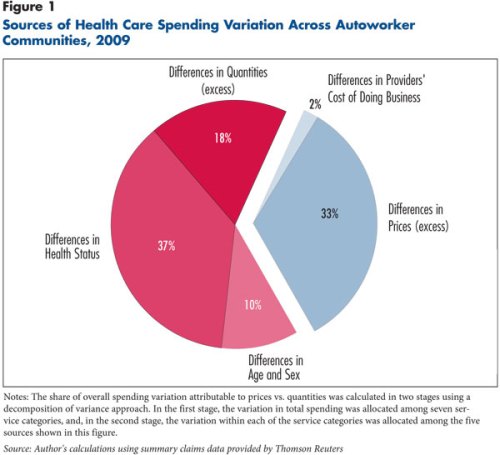

Difference in provider prices, particularly among hospitals, accounted for a third of the variation. Hospitals in Lake County, for instance, charged 2 1/2 times what Medicare paid, while hospitals in Syracuse charged 30 percent more than Medicare did. (The variation among doctors’ prices wasn’t nearly as great.)
The rest of the difference between the communities was due to the quantity of medical services used by the autoworkers and their families. The biggest contributing factor — making up 37 percent of the spending variation — was that the workers and families in the high-spending areas were in worse health than were their those in other regions.
Another 10 percent of the variation between communities was due to differences in the age and sex of the autoworkers and their families. (Older workers and females tend to have higher health care costs.) And 18 percent of the variation in utilization remained unexplained, such as in Cleveland, where the autoworkers were in about the same health as those in Syracuse, but Cleveland’s spending was substantially higher.
From this, the paper concludes that holding down costs probably can’t be done simply by making places that use lots of health care resources operate like low-quantity communities. “Taking an Akron or a Toledo and turning it into a Buffalo or a Syracuse would almost certainly require genuine improvements in health and health behaviors,” the paper’s author, Chapin White, writes.
The paper also found that the sickness levels of the autoworkers and their families tended to mirror the general health in their communities. Therefore, the paper suggests, policymakers need to focus on broad programs to improve health community-wide, and clamp down on the prices hospitals charge, either by altering insurance products, perhaps by creating tiered networks, or having the government review or set rates as Maryland does.
Here are the communities in the study with health spending per enrollee, listed in ascending order:
Buffalo: $4,500
Syracuse: $4,900
Rockford: $5,000
Grand Rapids, Mich.: $5,100
Youngstown, Ohio: $5,400
St. Louis: $5,400
Lansing, Mich.: $5,400
Wilmington, Del: $5,400
Saginaw, Mich.: $5,600
Warren, Mich.: $5,800
Monroe, Mich.: $5,800
Flint, Mich.: $5,900
Akron, Ohio: $6,000
Cleveland: $6,000
Toledo, Ohio.: $6,000
Detroit: $6,200
Kokomo, Ind.: $6,700
Indianapolis: $7,900
Lake County, Ill.: $9,000.