A major expansion is underway at the nation’s medical schools that will sharply increase the number of new physicians entering the workforce over the next decade to care for an aging Baby Boom generation. But critics say the move could backfire since medical schools are still channeling too many young doctors into highly paid specialties instead of primary care, which will exacerbate the problem of rising health care costs.
The Association of American Medical Colleges (AAMC) unveiled a new survey Thursday showing the number of students entering the nation’s 137 accredited medical schools will surge nearly 30 percent from 2002 levels to 21,376 in 2016, meeting a goal set in 2006 when it was widely believed an aging population would require far more physicians. About 19,638 first-year students will enter medical school this fall, up from 16,488 in 2002.
But the campaign to increase the number of practicing physicians, which has been spearheaded AAMC, has come under fire in recent years on two fronts. Health care reformers say the increased enrollment has not addressed the ongoing shortage of primary care physicians, especially in poor and rural areas, which will only grow worse when 30 million previously uninsured patients seek compensated care after 2014 because of the Affordable Care Act.
Meanwhile, cost-control advocates fret that the continuing migration of too many young physicians into highly paid specialties is contributing to the crisis in Medicare financing, which has been driven in part by overuse of expensive procedures. The AAMC projection assumes aging baby boomers, like their parents, will become more dependent on the specialists who treat heart disease, diabetes, cancer and other chronic conditions that become more prevalent as people age.
Officials at AAMC say they have taken both factors into account in making the projections that led to the major increase in medical school slots. A dozen new medical schools have opened in the U.S. since 2002, including four in Florida, and seven more have either applied or plan to apply for accreditation.
“If you’re less than 50 years old, the majority of your visits are to primary care physicians, but after you turn 65, the majority of visits are to specialists,” said Atul Grover, a physician and chief of public policy at AAMC. “With the over-65 population growing rapidly, we’re also going to have a shortage of specialists.”
AAMC, which tracks medical professionals for the first seven years after they finish school, estimates about a third of newly-minted doctors go into some form of primary care, either internal medicine, pediatrics or family practice. But researchers at the Center for Studying Health System Change (CSHSC) peg the total at closer to 20 percent since many internal medicine trainees eventually take up a specialty instead of remaining in general practice.
That career shift is often due to the skewed compensation schedules for practicing physicians, which are recommended by an American Medical Association committee (dubbed the Resource-Based Relative Value Scale Update Committee or RUC). It sets the relative worth of medical services, and values procedural tasks like inserting a vascular stent more highly than cognitive tasks like diagnosing a small child’s illness. As a result, family physicians, pediatricians and geriatricians are among the lowest paid, earning on average $200,000 per year or less.
Newly-minted specialists like surgeons, intervention cardiologists or radiologists who’ve completed their advance training, on the other hand, earn $300,000 or more to start and often earn two or three times that by the time they are in their mid-40s. American doctors are, by far, the most highly paid physicians in the world.
“Cardiology pays twice as much as primary care,” said Grover. “That’s a really hard incentive structure to fight against.”
As a result, “the U.S. has relied on foreigners to fill primary care jobs,” said Tracy Yee, a researcher at CSHSC. The U.S. attracts anywhere from 5,000 to 6,000 foreign-trained physicians a year, many coming from less-developed countries that have large unmet medical needs and face their own physician shortages.
“We’re doing to medicine what we’ve done to low-paid service jobs,” said Shannon Brownlee, acting director of health policy at the New America Foundation. “We’re filling the lowest paid physician jobs – primary care docs – with foreign doctors who should probably be treating people in their home countries.”
Architects of health care reform hope greater emphasis on coordinated care for people with chronic conditions through accountable care organizations and medical homes will create more and better-compensated jobs for primary care physicians. Larger organizations can also turn over routine tasks to physician assistants and nurse practitioners.
Some are also looking to growing ranks of women physicians to transform in the profession. They now take up half the slots in medical school and could produce over time a workforce more willing to sacrifice higher pay for the more regular hours of primary care.
A major shift into primary care from specialization would make sense, according to researchers associated with the Center for Health Policy Research at Dartmouth. Their research has shown that areas with greater numbers of specialists per Medicare beneficiary tend to have significantly higher costs per patient without any better outcomes.
A recent survey of Medicare beneficiaries conducted by Dartmouth and the Centers for Medicare and Medicaid Services and published last year in Health Affairs found patients living in areas with more physicians per capita perceived no differences in their access to health care than beneficiaries with fewer available physicians. Moreover, there were no differences between the two groups in terms of visits or time spent with their personal physician, the number of tests they received or the number of specialists they saw.
“Simply training more physicians is unlikely to lead to improved access to care,” the researchers concluded. “Instead, focusing health policy on improving the quality and organization of care may be more beneficial.”

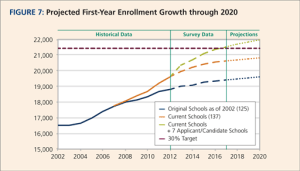
Source: Association of American Medical Colleges
?