

On the first morning of Jang Yeo Im’s vacation to San Francisco in 2016, her 8-month-old son, Park Jeong Whan, fell off the bed in the family’s hotel room and hit his head.
There was no blood, but the baby was inconsolable. Jang and her husband worried he might have an injury they couldn’t see, so they called 911, and an ambulance took the family — tourists from South Korea — to Zuckerberg San Francisco General Hospital (SFGH).
The doctors at the hospital quickly determined that baby Jeong Whan was fine — just a little bruising on his nose and forehead. He took a short nap in his mother’s arms, drank some infant formula and was discharged a few hours later with a clean bill of health. The family continued their vacation, and the incident was quickly forgotten.
Two years later, the bill finally arrived at their home: They owed the hospital $18,836 for a visit lasting three hours and 22 minutes, the bulk of which was for a mysterious fee for $15,666 labeled “trauma activation,” also known as “a trauma response fee.”


A photo of Park Jeong Whan at Zuckerberg San Francisco General Hospital after his admission shows bruise marks on the forehead and nose from his fall.(Jun Michael Park for Vox)
“It’s a huge amount of money for my family,” said Jang, whose family had travel insurance that would cover only $5,000. “If my baby got special treatment, OK. That would be OK. But he didn’t. So why should I have to pay the bill? They did nothing for my son.”
American hospital bills are today littered with multiplying fees, many of which don’t even exist in other countries: fees for blood draws, fees for checking the blood oxygen level with a skin probe, fees for putting on a cast, minute-by-minute fees for lying in the recovery room.
But perhaps the pinnacle is the “trauma fee,” in part because it often runs more than $10,000 and in part because it seems to be applied so arbitrarily.
A trauma fee is the price a trauma center charges when it activates and assembles a team of medical professionals that can meet a patient with potentially serious injuries in the ER. It is billed on top of the hospital’s emergency room physician charge and procedures, equipment and facility fees.
Emergency room bills collected by Vox and Kaiser Health News show that trauma fees are expensive and vary widely from one hospital to another.

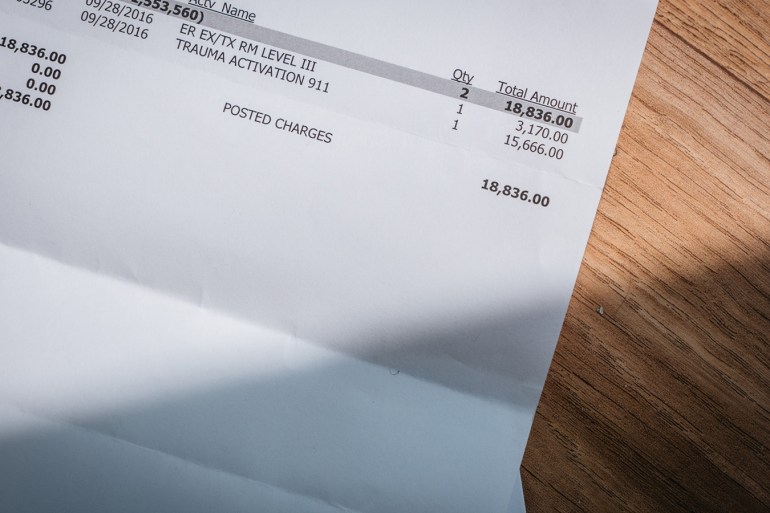
The medical bill for $18,836 from Zuckerberg San Francisco General Hospital. (Jun Michael Park for Vox)

The Jang family near their apartment complex in Suwon, an hour south of Seoul, South Korea. (Jun Michael Park for Vox)
Charges ranged from $1,112 at a hospital in Missouri to $50,659 at a hospital in California, according to Medliminal, a company that helps insurers and employers around the country identify medical billing errors.
“It’s like the Wild West. Any trauma center can decide what their activation fee is,” says Dr. Renee Hsia, director of health policy studies in the emergency medicine department at the University of California-San Francisco.
Hsia is also an emergency medicine doctor at Zuckerberg San Francisco General Hospital, but was not involved in the care of the patients discussed in the story — and spoke about the fees generally.
Comprehensive data from the Health Care Cost Institute shows that the average price that health insurers paid hospitals for trauma response (which is often lower than what the hospital charges) was $3,968 in 2016. But hospitals in the lowest 10 percent of prices received an average of $725 — while hospitals in the most expensive 10 percent were paid $13,525.
Data from Amino, a health cost transparency company, shows the same trend. On average, Medicare pays just $957.50 for the fee.
According to Medicare guidelines, the fee can be charged only when the patient receives at least 30 minutes of critical care provided by a trauma team — but hospitals do not appear to be following that rule when billing non-Medicare patients.
At the turn of the century such fees didn’t even exist.
But today many insurers willingly pay them, albeit at negotiated rates for hospitals in their networks. Six insurers and industry groups declined to discuss the fees, and a spokeswoman for America’s Health Insurance Plans, the industry trade group, said, “We have not seen any concerning trends surrounding trauma center fees.”
Trauma centers argue that these fees are necessary to train and maintain a full roster of trauma doctors, from surgeons to anesthesiologists, on-call and able to respond to medical emergencies at all times.
SFGH spokesman Brent Andrew defended the hospital’s fee of over $15,000 even though the baby didn’t require those services.
”We are the trauma center for a very large, very densely populated area. We deal with so many traumas in this city — car accidents, mass shootings, multiple vehicle collisions,” said Andrew. “It’s expensive to prepare for that.”
At What Cost Trauma?
Experts who’ve studied trauma fees say that at some hospitals there’s little rationale behind how hospitals calculate the charge and when the fee is billed. But, of course, those decisions have tremendous financial implications.
After Alexa Sulvetta, a 30-year-old nurse, broke her ankle while rock climbing at a San Francisco gym in January, she faced an out-of-pocket bill of $31,250 bill.
An ambulance also brought Sulvetta to Zuckerberg San Francisco General Hospital, where, she recalled, “my foot was twisted sideways. I had been given morphine in the ambulance.”
Sulvetta was evaluated by an emergency medicine doctor and sent for emergency surgery. She was discharged the next day.

Alexa Sulvetta and her husband, Ben Verley, at their home in Oakland, Calif.(Heidi de Marco/KHN)
SFGH also charged Sulvetta a $15,666 trauma response fee, a hefty chunk of her $113,338 bill. Her insurance decided that the hospital fees for the one-day stay were too high, and — after negotiations — agreed to pay only a charge it deemed reasonable. The hospital then went after Sulvetta for $31,250.
“My husband and I were starting to think about buying a house, but we keep putting that off because we might need to use our life savings to pay this bill,” she said.
SFGH spokesman Andrew, meanwhile, said that the hospital is justified in pursuing the bill. “It’s fairly typical for us to pursue patients when there are unpaid balances,” he said. “This is not an uncommon thing.”
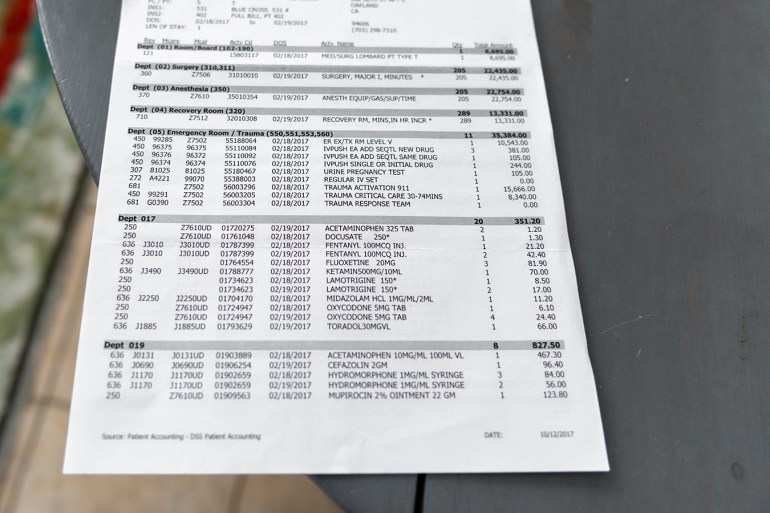
Alexa Sulvetta’s hospital bill, including the $15,666 trauma response fee. (Heidi de Marco/KHN)

Ben Verley points out his wife’s scar, left after she broke her ankle rock climbing at a San Francisco gym. (Heidi de Marco/KHN)
‘I Feel Like I Created A Monster’
Trauma response fees were first approved by the National Uniform Billing Committee in January 2002, following a push by a national consulting firm specializing in trauma care. The high costs of staffing a trauma team available at all hours, the firm argued, threatened to shut down trauma centers across the country.
Trauma centers require special certification to provide emergency care for patients suffering very serious injuries above and beyond a regular emergency department.
“We were keeping an ongoing list of trauma centers that were closing all over the country,” said Connie Potter, who was executive director of the firm that succeeded in getting the fee approved. She now consults with hospital trauma centers on how to bill appropriately.
Trauma teams are activated by medics in the field, who radio the hospital to announce they are arriving with a trauma patient. The physician or nurse who receives the call then decides whether a full or partial trauma team is needed, which results in different fees. Potter said that person can also activate the trauma team based on the consultation with the EMTs.
But reports from the field are often fragmentary and there is much discretion in when to alert the trauma team.
An alert means paging a wide range of medical staff to stand at the ready, which may include a trauma surgeon, who may not be in the hospital.
Potter said if the patient arrives and does not require at least 30 minutes of critical care, the trauma center is supposed to downgrade the fee to a regular emergency room visit and bill at a lower rate, but many do not do so.
Hospitals were supposed to come up with the fee for this service by looking at the actual costs of activating the trauma team, and then dividing it over the amount that their patients are likely to pay. Hospitals that see a lot of uninsured and Medicaid patients might charge more to patients with private insurance to make up for possible losses.
But soon, Potter said, some hospitals began abusing the fee by charging an exorbitant amount that seemed to be based on the whims of executives rather than actual costs.
“To a degree, I feel like I created a monster,” Potter said. “Some hospitals are turning this into a cash cow on the backs of patients.”
The $15,666 is San Francisco General’s low-level trauma response fee. The high-level response fee in which the trauma surgeon is called into action is $30,206. The hospital would not provide a breakdown of how these fees are calculated.
Unfortunately, outside of Medicare and state hospitals, regulators have little sway over how much is charged. And at public hospitals, such fees may be a way to balance government budgets. At SFGH, the $30,206 higher-level trauma response fee, which increased by about $2,000 last year, was approved by the San Francisco Board of Supervisors.
An Ibuprofen, Two Medical Staples — And A $26,998 Bill
Some patients question whether their particular cases ought to include a trauma fee at all — and experts think they’re right to do so.
Sam Hausen, 28, was charged a $22,550 trauma response fee for his visit to Queen of the Valley Medical Center in Napa, Calif., in January.
An ambulance brought him to the Level 3 trauma center after a minor motorcycle accident, when he took a turn too quickly and fell from his bike. Records show that he was alert with normal vital signs during the 4-mile ambulance ride, and that the ambulance staff alerted the hospital that the incoming patient had traumatic injuries.
He was at the hospital for only about half an hour for a minor cut on his head, and he didn’t even need X-rays, CAT scans or a blood test.

Sam Hausen was charged a $22,550 trauma response fee for his visit to Queen of the Valley Medical Center in Napa, Calif., after a motorcycle accident.(Heidi de Marco/KHN)
“The only things I got were ibuprofen, two staples and a saline injection. Those were the only services rendered. I was conscious and lucid for the whole thing,” said Hausen.
But because the ambulance medics called for a trauma team, the total for the visit came to $26,998 — and the vast majority of that was the $22,550 trauma response fee.
Queen of the Valley Medical Center defended the charge. “Trauma team activation does not mean every patient will consult with and/or be cared for by a trauma surgeon,” spokeswoman Vanessa deGier said over email. “The activation engages a team of medical professionals. Which professional assesses and cares for a trauma patient depends on the needs and injury/illness of the patient.”
Guidelines for trauma activation are written broadly on purpose, in order to make sure they don’t miss any emergencies that could otherwise kill patients, said Dr. Daniel Margulies, a trauma surgeon at Cedars-Sinai in Los Angeles and chair of the American College of Surgeons committee on trauma center verification and review. Internal injuries, for example, can be difficult to diagnose at the scene of an accident.
“If you had someone who needed a trauma team and didn’t get called, they could die,” he said.
Medics err on the side of caution when calling in trauma patients to avoid missing a true emergency. To that end, the American College of Surgeons says it is acceptable to “overtriage,” summoning the trauma team for 25-35 percent of patients who don’t end up needing it.
But that logic leaves health consumers like Jang, Sulvetta and Hausen with tens of thousands in potential debt for care they didn’t ask for or need, care that is ordered out of an abundance of caution — a judgment call by an ambulance worker, a triage nurse or a physician — based on scant information received over a phone.
Jeong Whan had fallen 3 feet from a hotel bed onto a carpeted floor when his nervous parents summoned an ambulance. By the time the EMTs arrived, Jeong Whan was “crawling on the bed, not appearing to be in any distress,” according to the ambulance records. The EMTs called SFGH and, after a consultation with a physician, transported Jeong Whan as a trauma patient, likely because of the baby’s young age.
At the hospital, Jeong Whan was evaluated briefly by a triage nurse and sent to an emergency department resuscitation bay.
Jang recalls being greeted by nine or 10 providers at the hospital, but the baby’s medical records from the visit do not mention a trauma team being present, according to Teresa Brown of Medliminal, who reviewed the case.

Jeong Whan was discharged with a clean bill of health after staying at Zuckerberg San Francisco General Hospital for a couple of hours. Jang Yeo Im claims that he didn’t receive any medical treatment at the hospital and she put the Band-Aid on her son’s nose herself.(Jun Michael Park for Vox)
The baby appeared to have no signs of major injury, and no critical care was required. Five minutes later, the family was transferred to an exam room for observation before being released a few hours later. Brown said she would dispute the $15,666 trauma response fee because the family does not appear to have received 30 minutes of critical care from a trauma team.
Jang currently has a patient advocate working on her behalf to try to negotiate the bill with the hospital. She said she fears that the pending medical debt could prevent her from getting a visa to visit New York and Chicago, which she hopes to do in the next few years.
She said her experience with the U.S. health care system and its fees has been shocking. “I like the USA. There are many things to see when traveling,” she said. “But the health care system in USA was very bad.”
This story was produced in collaboration with Vox, which is collecting emergency room bills as part of a year-long project focused on American health care prices.
KFF Health News’ coverage of children’s health care issues is supported in part by the Heising-Simons Foundation.