



This story also ran on InvestigateTV. It can be republished for free.
Debbie Cook was in her pajamas on a summer morning in 2019 when she got a call from her son: “Something bad is wrong with Granny.”
The fear in his voice told Cook it was serious. She dialed 911 immediately, knowing it could take time for an ambulance to navigate the country roads in Fentress County, Tennessee.
She got dressed and made the short drive across the family farm, over two bridges and a creek, to her mother’s house. Cook prayed that one of the three ambulances covering their roughly 500-square mile county was near.
When Cook arrived, she found her mother, Lottie Crouch, in the bathroom, unable to stand or walk. Cook, a licensed practical nurse, quickly recognized the signs: lopsided face, one side of the mouth drooping.
Her mama was having a stroke.
“I was petrified,” Cook recalled. She started her career working with stroke rehab patients and knew that getting the right care fast could mean life or death. Or a big difference in her mother’s quality of life. Crouch was 75 and still energetic and loved doing things like firing up a kettle of soup for herself. To continue living the life Crouch knew, each step toward getting care in a rural area had to go right.
But when the paramedics arrived, one of the biggest questions was: Where would they take Crouch for care?

Across the nation, nearly 800,000 people suffer strokes each year. The issue is particularly acute across the regions of Appalachia and the Mississippi Delta, where more than 80% of counties have stroke death rates above the national average. Many of these counties also face high rates of poverty and are home to vulnerable elderly populations. They have a shortage of medical providers or have seen local hospitals shutter.
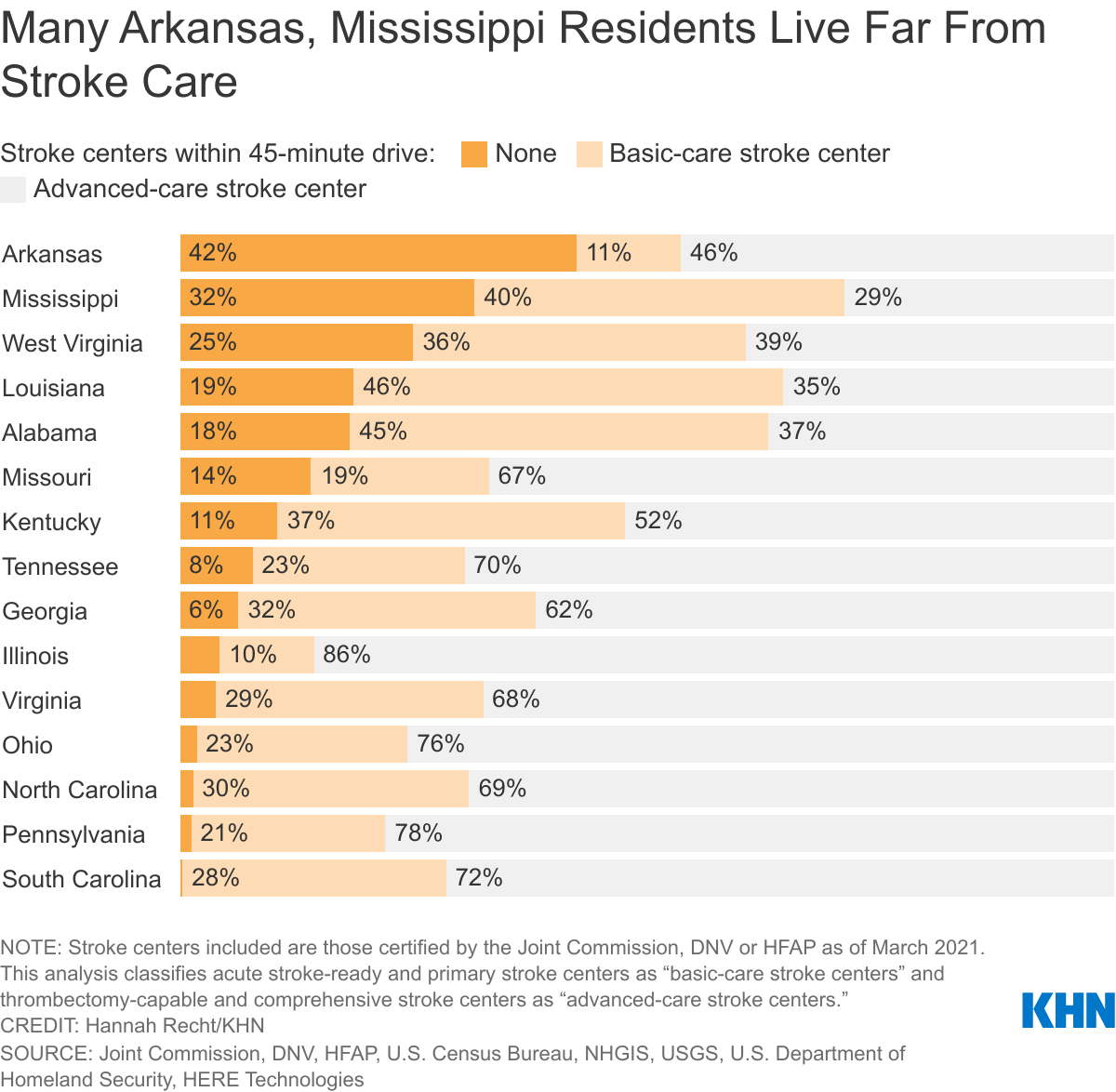
In Tennessee, 2 million people — nearly one-third of the state — are people like Crouch who live more than 45 minutes from a hospital that is stroke-certified and able to provide the most advanced care, according to a new analysis by KHN and InvestigateTV. And rates are even higher in Delta states such as Arkansas and Mississippi, where more than half of residents must drive longer than 45 minutes to those specialized stroke centers.

The analysis is part of a yearlong project called Bridging the Great Health Divide, in which KHN and Gray Television’s national investigative team, InvestigateTV, are digging into health issues that have historically plagued these regions. Strokes are chief among them. Despite medical advancements in stroke care, routing patients from rural parts of Appalachia and the Delta to the appropriate facility is an intricate jigsaw puzzle.
Localize The Data
Proximity to stroke-certified hospitals and county stroke death rates
Download The Data“There’s not the same one correct answer for all patients,” said Dr. Raul Nogueira, an interventional neurologist at Grady Memorial Hospital in Atlanta. Where a patient should be taken for care “really depends on travel time,” he said. “It’s all about time.”
For years, the advice for stroke patients has been to get to the nearest hospital as soon as possible. A stroke cuts off blood flow to part of the brain, and the sooner that blood flow can be restored the better. So, the idea has been to get patients to a doctor — any doctor — quickly.
But that advice is now evolving. Research shows some stroke patients benefit more from advanced procedures typically done by specialists at large medical centers. The new goal is to get patients to the right doctor at the right hospital as soon as possible.
In some cases, that means skipping the closest facility. For patients with severe strokes, in which a clot is blocking one of the brain’s major arteries, the American Heart and Stroke associations recommend traveling up to an additional 30 minutes in urban areas and 60 minutes in rural areas to reach a hospital with more advanced stroke capabilities.
While that’s easy enough in a city where multiple hospitals are clustered together, in rural areas like Fentress County the question of where to take a patient has become increasingly fraught.
Big Decisions, Little Time
When Lottie Crouch had her stroke, what would have been the nearest hospital, less than 20 minutes away, had closed two months earlier. It’s one of 136 rural hospitals nationwide that have shuttered since 2010, including nearly three dozen across Appalachia and the Delta. That meant the closest in-state hospital for Crouch was nearly 45 minutes away by car, and medical centers with the most advanced care were more than an hour’s drive. That left EMS services stretched thin trying to transport patients farther away.
Each step in the process to get someone who’d had a stroke to the right care within the right amount of time had become more complex.
The decisions along the way are rarely clear-cut, Nogueira said. If a patient has a severe stroke, they might benefit from getting to a large medical center where they can undergo surgery right away, he said. Stopping at a smaller hospital that can’t perform that procedure might unnecessarily delay care.
But if the stroke is less severe, the person might benefit more from first going to a closer facility that can offer medications to break up the clot sooner, Nogueira said. Then the patient could avoid unnecessary medical bills from a long trip, anything from $500 for a ride in the back of a regular ambulance to $50,000 for a helicopter. And their family could save the time and money needed to visit them in a faraway hospital.
The problem is that first responders can’t necessarily tell how severe a stroke is just by looking at someone. So, they rely on an evaluation of the patient’s symptoms to make the best choice.
The gravity of these decisions weighs on Jamey Beaty, a paramedic in Fentress County, who responded to Lottie Crouch’s home.
“When you’re in the back of a truck and all alone and you have a patient actively dying on you, the only thing you can think about is: How can I keep this patient alive until I can get them somewhere?” Beaty said. “That’s all that crosses your mind.”
Anytime Beaty gets a call about a stroke, his first response is to look at the sky.
Since the local hospital closed, an air ambulance is how he quickly gets people to treatment. The day Lottie Crouch had her stroke, luckily the Tennessee sky was clear blue. Crouch was taken nearly 100 miles to a hospital in Knoxville with advanced stroke services.

Long Journeys to Advanced Care
Over the past two decades, two main treatments have advanced care for strokes caused by a blockage — the most common type of stroke in America. The first is a medication delivered through an IV to break up clots in patients’ blood vessels. The medicine has to be given within 4½ hours of when symptoms start. The second is a procedure using a catheter to physically remove the clot from a patient’s vessels. This treatment can be done up to 24 hours after symptoms start but is generally used only for severe strokes.
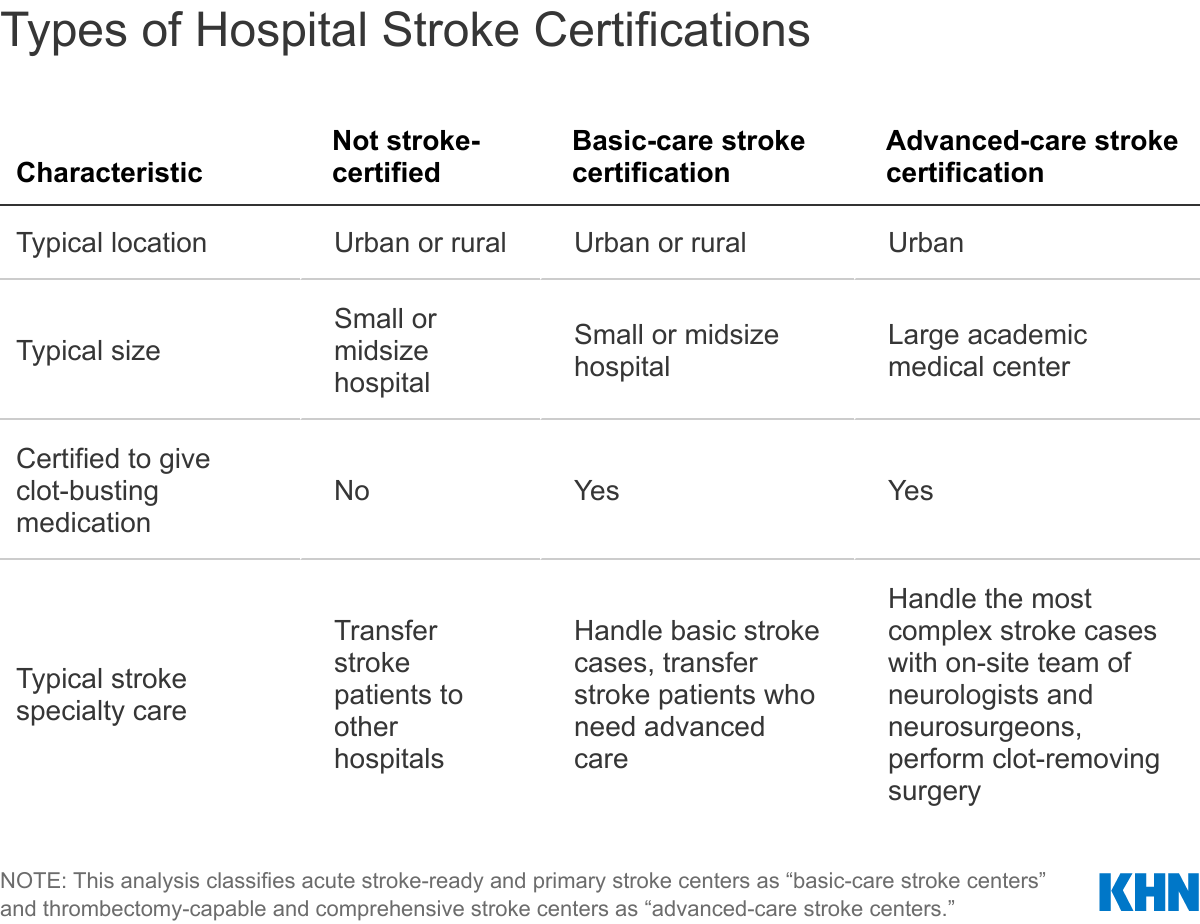
Across the country, hospitals are certified by tiers, largely based on their ability to regularly provide these treatments. Some hospitals have no certification. Among stroke-certified hospitals, the first level is acute stroke-ready hospitals, which can assess stroke patients, keep them stable and provide clot-busting medications. At the other end of the spectrum are comprehensive stroke centers, which have specialized teams of neurologists and neurosurgeons. In addition to giving the clot-busting drugs, these centers can physically remove clots.

The big question is: Which facility can and should stroke patients be taken to first to get the right care within the right time span?
In Appalachia, about 11% of residents must drive more than 45 minutes to reach any kind of stroke center, according to the KHN and InvestigateTV analysis. That proportion is even higher in the Delta, where nearly a third of residents have to drive more than 45 minutes to a stroke center. Another third of Delta residents have only basic-care stroke centers within that distance and would need to drive farther for advanced stroke surgeries.
And in the most rural parts of both these regions, people are less likely to be near an advanced-care stroke facility.


Rural and Largely African American
While reaching appropriate stroke care in time is difficult for many rural Americans, such as Crouch, who is white, the concerns are compounded for places with a large Black population.
Black Americans have strokes more often and at younger ages than their white counterparts. They’re also less likely to receive clot-busting medications because they often arrive at the hospital outside the window of treatment.
In Sumter County, Alabama, several people interviewed — from a business owner to a college professor to the district judge — were able to name someone off the top of their heads who has had a stroke. The county is more than 70% Black, and it is one of the poorest areas of the state.
The only hospital within county lines has no stroke certification. Loretta Wilson, the CEO of Hill Hospital of Sumter County, wishes her facility could do more for stroke patients. But clot-busting medications can cost $8,000 per dose, and the hospital can’t always afford to keep them on hand, she said.
Most stroke patients are taken to larger hospitals at least 30 or 40 minutes away. That can be a long and expensive journey for many residents, Wilson said.
Signs of a Stroke
F — Face: Ask the person to smile. Does one side of the face droop?
A — Arms: Ask the person to raise both arms. Does one arm drift downward?
S — Speech: Ask the person to repeat a simple phrase. Is the speech slurred or strange?
T — Time: If you see any of these signs, call 911 right away.
Source: https://www.cdc.gov/stroke/signs_symptoms.htm
Understanding that, Wilson focuses largely on prevention efforts. She runs a nonprofit that tackles issues like high blood pressure, obesity and diabetes, all of which increase a person’s risk of stroke. Her organization partners with churches to teach people about healthy eating and exercise, and passes around blood pressure monitors so congregants can screen themselves after services.
“We have a high African American population,” said Wilson, who is African American too, “and those are the ones who really need the services.”
Other organizations in the county also work to educate people about heart health and when to call 911. The local college’s nursing program has a scholarship aimed at bringing more medical providers to the area.
Using Telestroke to Boost Rural Care
In rural hospitals, even if doctors have access to clot-busting drugs, they may hesitate to administer them for fear of harming the patient. In rare instances — about 2% to 7% of cases — the drugs can cause bleeding in the brain.
But not using the drugs can also have consequences. A national study published in 2020 found stroke patients were less likely to receive those medications in rural hospitals than urban ones, and stroke patients were more likely to die in rural hospitals.
Telestroke programs can help bridge that gap, said Dr. Amelia Adcock, a neurologist at WVU Medicine in West Virginia and head of the system’s telestroke network.
By connecting doctors from smaller, often rural, hospitals with an on-call specialist at a large medical center, the programs allow people “to share the burden of decision-making,” Adcock said. And the liability.
Dr. Michael Gould is an emergency medicine doctor at the 25-bed Potomac Valley Hospital in rural northern West Virginia. His hospital is not stroke-certified and does not have a neurologist on staff. He said giving clot-busting drugs is “one of the decisions in medicine that makes me the most nervous.”
But consulting with neurologists at WVU Medicine’s hub about 80 miles away in Morgantown has given him more confidence, he said. Gould estimated he now administers the drugs once or twice a month.
A study of WVU Medicine’s telestroke network found the number of stroke patients receiving clot-busting medications nearly doubled over the first three years of the program.
Last fall, Christopher Green was picking up groceries when he suddenly developed a severe headache and lost his peripheral vision. Green, a longtime paramedic, immediately recognized what was happening. “Oh, my God, I’m having a stroke,” he remembers thinking. He was brought to Gould’s hospital, and the ER staff immediately fired up the telestroke program.

Within 30 minutes, Green got drugs to break up the blockage in his vessels. “A textbook outcome,” said Green, who has responded to many 911 calls for stroke.
Looking back, Green said he probably would have taken a patient in his situation to a farther hospital that was stroke-certified. But experiencing the telestroke program firsthand changed his outlook.
”Now I see that delaying that treatment 20 to 30 minutes makes a difference on whether you have a full resolution or some kind of residual effects,” he said.
‘What Could It Have Been?’
Back in Tennessee, Debbie Cook was grateful her mother was taken to the advanced-care stroke center in Knoxville. It allowed Lottie Crouch to get the treatment she needed so she can still lead a mostly independent life.
But there were trade-offs. The distance took a toll on the family. Cook, her sister and her daughter took turns driving nearly two hours each way to watch over Crouch in the hospital each night.
After 10 days, when Crouch was transferred to a rehab facility closer to home, the family felt a sense of relief. They could bring her meatloaf and wild blackberry dumplings for dinner. And “a lot of peppermint candy,” Crouch recalled — her favorite.
Although Crouch is now healthy and at home, her 27-year-old granddaughter, Haelee Stockton, is still haunted by the possibility of what could have happened that day. If the paramedics hadn’t made it in time or if bad weather had prevented the helicopter from flying, her granny might not be alive.
“What could it have been?” Stockton said. “How lucky was she? And how many people are going to get that lucky in the future?”

Aneri Pattani led the reporting and writing for this story. Hannah Recht led the data analysis and graphics. InvestigateTV’s Daniela Molina contributed to this report.
Read the methodology to learn how we did this analysis and visit the Github repository to see the code.