
This story also ran on Fortune. It can be republished for free.
Health insurers and medical providers are battling over who should supply high-cost infusion drugs for patients, with the tussle over profits now spilling into statehouses across the country.
The issue is that some insurers are bypassing hospital pharmacies and physician offices and instead sending more complex drugs through third-party pharmacies. Those pharmacies then send the medications directly to the medical provider or facility for outpatient infusing, which is called “white bagging,” or, more rarely, to patients, in what is called “brown bagging.” That shifts who gets to buy and bill for these complex medications, including pricey chemotherapy drugs.
Insurers say the policies are needed because hospital markups are too high. But hospitals argue that adding an intermediary results in unnecessary risks and delays, and they say some insurers have their own or affiliated pharmacy companies, creating financial motives for controlling the source of the medications. The patients, meanwhile, are left to deal with the red tape.
Paula Bruton Shepard in Bolivar, Missouri, is among those caught in the middle. Flares of lupus, an autoimmune disease, rob Shepard of her mobility by attacking her joints. She relies on monthly infusions to treat her symptoms. But at times, she said, her treatments were delayed due to UnitedHealthcare’s white bagging infusion policy. And interruptions to her treatments exacerbated her symptoms.
“I once had to use a toilet lift and it was kind of demoralizing to say, ‘I’m a 50-year-old woman and I have to use a toilet lift,’” Shepard said of the medication delays.
This is a tug of war over profits between insurers and medical providers, said Ge Bai, a professor of accounting and health policy at Johns Hopkins University. While insurers claim the arrangement reduces costs, she said, that doesn’t mean insurers pass along savings to patients.
“I don’t think we should have more sympathy toward one party or the other,” Bai said. “Nobody is better than the other. They’re all trying to make money.”
The savings from white bagging can be significant for expensive infusion drugs, according to a report from the Massachusetts Health Policy Commission. For example, Remicade, used to treat a variety of inflammatory diseases, including Crohn’s, cost on average $1,106 per unit in 2015 under hospitals’ traditional buy-and-bill system, the commission found in its review of state claims data. That same drug cost an average of $975 per unit under white bagging, a 12% savings.
But the report also found patients, on average, faced higher cost sharing — what they are responsible for paying — for Remicade and other drugs when white bagging was used. While some patients had only modest increases to their costs under the policy, such as $12 more for a medication, the review found it could mean much greater cost sharing for some patients, such as those on Medicare.
At Citizens Memorial Hospital in rural Bolivar, more than 1 in 4 patients who receive regular infusions are being forced to use an outside pharmacy, said Mariah Hollabaugh, the hospital’s pharmacy director. Shepard was among them.
Even if the hospital has the exact drug on the shelf, patients must wait for a separate shipment, Hollabaugh said, potentially interrupting care. Their shipped drugs may sometimes be unusable when the doctor needs to change the dosage. Or the medicine comes in a nondescript package that doesn’t get immediately flagged for the pharmacy, potentially subjecting the drugs to damaging temperature fluctuations. For patients, that can mean delays in care.
“They’re in pain, they’re uncomfortable,” Hollabaugh said. “They may be having symptoms that don’t allow them to go to work.”
Siteman Cancer Center, led by physicians from Washington University School of Medicine in St. Louis, has confronted the same issue. But the cancer center’s size has helped it largely avoid such insurer policies.
John DiPersio, a Siteman oncologist and researcher who led the university’s oncology division for more than two decades, said Siteman reluctantly allows white bagging for simple injectables but refuses to accept it for complicated chemotherapies. It does not accept brown bagging. Occasionally, he said, that means turning patients away.
“You’re talking about cancer patients that are getting life-threatening treatments,” DiPersio said, referring to the dangers of chemo drugs, which he said can be fatal if used improperly. “It doesn’t make any sense to me. It’s all stupid. It’s all lunacy.”
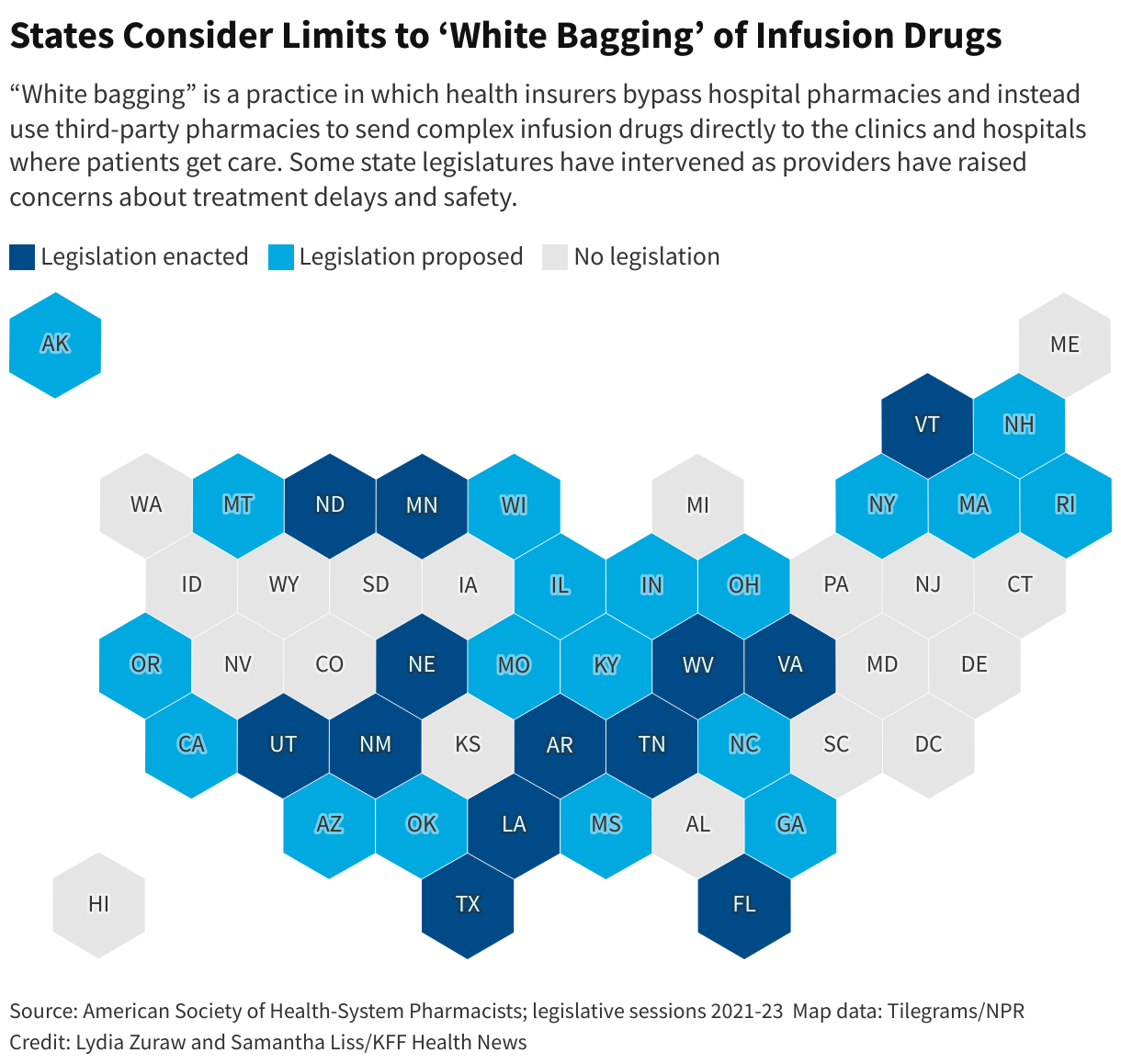
At least 21 states, including Missouri, introduced some form of white or brown bagging legislation during the most recent legislative session, according to the American Society of Health-System Pharmacists. And in the past two years, the trade group said, at least 13 states have already enacted restrictions on white bagging, including Arkansas, Louisiana, and Virginia.
ASHP has created model legislation to limit insurers from requiring the practices as a condition of coverage.
“This is a major issue,” said Tom Kraus, a vice president at the trade group. “We see this as central to our ability to coordinate patient care.”

At the heart of the tension is an often-litigated federal program that allows certain hospitals and the clinics they own to purchase drugs at deep discounts. The 340B program, named for a section of the law that created it, allows hospitals to buy certain drugs for much less — sometimes for a total cost of a single penny — than what they are later paid for those drugs. Hospitals are not required to pass along 340B savings to patients.
The program was intended to help hospitals spread scarce resources further to treat patients in poor and vulnerable communities, but it has morphed into a means of enriching hospitals and their affiliated clinics, researchers said in a 2014 Health Affairs report. Hollabaugh said many rural facilities such as Citizens rely on the revenue generated from the 340B drugs to subsidize infusions that have no profit margin.
The number of participating hospitals and their affiliated outpatient clinics has increased significantly since the 340B program was created in 1992. More than 2,600 of the nation’s roughly 6,100 hospitals were participating in the 340B program as of January 2023. That gives them access to discounts that can knock off as much as 50% of a drug’s cost, according to the Health Resources & Services Administration, which oversees the program.
The insurance industry argues that hospital markups, especially when made on top of those discounts, have gotten out of control.
“The fact is, people got greedy,” Shannon Cooper, a lobbyist for Blue Cross and Blue Shield of Kansas City, said during a Missouri state Senate hearing in March.
Markups are not unique to 340B hospitals, said Sean Dickson, who helps lead pharmaceutical policy for AHIP, a trade group formerly known as America’s Health Insurance Plans. The markups thrusted on commercial plans are “widely out of line” with what Medicare will pay, he said, and that is driving up costs without providing additional value.
Legislation that targets white bagging hinders an insurer’s ability to rein in such costs, Dickson said, especially when an area lacks competition.
“What we’re really trying to focus on here is putting pressure on those markups that are not related to cost or safety,” Dickson said.
Anthem Blue Cross and Blue Shield lobbyist David Smith testified during the March hearing in Missouri that even the idea of white bagging elicited a quick response and that almost every major hospital system in the state said they would drop their prices and come back to the negotiation table.
For now, Citizens Memorial Hospital and other Missouri medical facilities will have to continue to tango with the insurers: Legislation to limit white and brown bagging did not pass during the Missouri General Assembly’s recent session.


Shepard, though, won’t need such legislation.
UnitedHealthcare had been sending her lupus infusion through other pharmacies on and off since 2021, unwilling to cover the drugs if they came from Citizens’ in-house pharmacy. Shepard had to authorize each shipment before it was sent. If she missed the monthly call, she said, it was a “bureaucratic mess” trying to get the medication shipped.
“We are driving unnecessary costs out of the health care system to help make care more affordable, while also maintaining drug safety, effectiveness and quality of care,” UnitedHealthcare spokesperson Tony Marusic wrote.
But after KFF Health News inquired about Shepard’s case, Marusic said UnitedHealthcare stopped white bagging Shepard’s medication to “prevent potential delays in shipping.” And during her latest infusion in June, her hospital was again able to supply Shepard’s medication directly.
“I’m just so relieved,” Shepard said. “I don’t have to take phone calls. I don’t have to reply to emails. I just show up.”