For years, states have struggled to raise the quality of care in nursing homes using a regulatory stick – citations, fines and other sanctions when serious problems are discovered.


Irene DuRell, 82, works on what she calls a German star by intricately folding strips of paper together in the activity center of Welcome Nursing Home in Oberlin, Ohio in July. DuRell first learned to make the stars in 1953 and has been teaching anyone who wants to learn ever since. (Photo by Tim Harrison/For USA Today and KHN).
Last month Ohio began adopting a distinctly different, carrot-like approach – financial incentives that encourage better services for frail seniors.
It’s the latest effort to address longstanding concerns in nursing homes such as too few nurses, too many patients who develop painful bed sores or infections and too much staff turnover. While many facilities provide excellent care many others fall short, experts say.
Under Ohio’s new approach, almost 10 percent of the Medicaid payments to nursing homes will depend on factors including residents’ satisfaction, rates of medical complications and the number of nurses on staff. Seven other states have programs of this sort, but Ohio’s will be the largest. (Medicaid, a federal-state health program for low-income people, is the largest funder of nursing home services in the nation.)
Meanwhile, Medicare, the federal health plan for seniors, plans to roll out a similar program for nursing homes nationally over the next several years, after government officials evaluate results of a three-year demonstration project in Arizona, New York and Wisconsin that ended July 1. (Medicare pays for short nursing home stays for some patients who need skilled care after a hospitalization.)
Whether the strategy, which is also being used with hospitals by Medicare and other insurers, will improve nursing home care is far from certain. While the notion of rewarding facilities for providing quality care is attractive, early experiments along these lines have had little success.
“A number of states have attempted this but most programs have been short-lived and haven’t really made much of a difference,” said David Grabowski, a professor of health policy at Harvard Medical School and lead investigator for the Medicare demonstration project.
That may reflect shortcomings with the way programs have been designed rather than the failure of the underlying concept, several experts suggest.
“There is a lot of room to improve the way programs are structured and to maximize their impact,” said Dr. Rachel Werner, an associate professor of medicine at the University of Pennsylvania and author of an unpublished study examining the effectiveness of states’ nursing home “pay-for-performance” efforts.

DuRell walks the hallways of Welcome Nursing Home with the help of Administrator Jill Herron Monday in Oberlin, Ohio (Photo by Tim Harrison/For USA Today and KHN).
Currently, nursing homes are paid a flat daily rate no matter how well or poorly they treat patients – a system that “does not provide strong incentives for furnishing high quality care,” according to a recent report to Congress by the U.S. Dept. of Health and Human Services.
States such as Colorado, Georgia, Kansas, Nevada, Oklahoma, Utah and Vermont have tried to change that by awarding a small bonus (from 60 cents to $6.16 per day) if facilities achieve various standards. But industry representatives say those incentives are insufficient to generate significant enthusiasm for altering the status quo, according to Nicholas Castle, who has surveyed nursing home administrators and is a professor of health policy at the University of Pittsburgh.
Also, administrators question whether the right measures of performance are being used: only 17 percent said their state’s system used “appropriate quality indicators,” according to Castle’s unpublished report.
Ohio’s new program addresses the financial concern with much larger incentive payments. The state has 970 nursing homes and its Medicaid program spends $4.5 billion on long-term care.
Previously, Ohio offered a small incentive bonus – 1.7 percent of the daily rate. Now, nearly 10 percent of a nursing home’s daily Medicaid payments (up to $16.44 a day for each patient) depends on the facility meeting five of 20 quality standards. If that goal is achieved, the full rate is received; if not, some of the money is withheld.
Ohio’s approach provides a “much more powerful incentive” for facilities to take a close look at their operations, said Michael Cheek, vice president of long-term care policy at the American Health Care Association, an industry trade group.
Also, standards being used in Ohio to assess performance now include measures that address nursing home residents’ freedom to make their own choices, such as when they bathe or get up in the morning; how and when they take meals; and whether they have the chance to discuss their goals of care and their end-of-life preferences.
Other standards relate to patient and family satisfaction (both are extensively monitored through annual surveys in Ohio), staffing levels, environmental concerns, regulatory deficiencies and clinical measures such as pain or bed sores.
The goal of the initiative, as well as a broader health care overhaul launched last year by Republican Gov. John Kasich, is to create a “coordinated, comprehensive, patient-centered health care system in Ohio” that “reimburses for quality” and lowers the sharply rising trajectory of health care costs, explained Bonnie Kantor-Burman, director of the Ohio Department of Aging.
First, faced with an $8 billion state budget deficit, the governor pushed through significant cuts to Medicaid in last year’s two-year budget, including slashing nursing home rates by $360 million.
“We’re dealing with a very challenging environment” but Ohio’s nursing homes generally support the state’s new quality initiative, in part because most will qualify for new, quality-based incentive payments without much trouble, said Peter Van Runkle, executive director of the Ohio Health Care Association.
The threshold for receiving those payments has been the most controversial element of the state’s plan, with some observers arguing that the bar was set too low to result in any meaningful improvement.
“It just doesn’t seem that (nursing homes) will have to stretch themselves enough, and I’ll be advocating for raising the threshold in the future,” said Beverley Laubert, Ohio’s long-term care ombudsman. Initially, she had advocated that homes meet 15 of 20 standards, a goal that many would have found difficult to achieve.
“This system rewards performance at a minimum level, not excellence,” said John Alfano, president of Leading Age Ohio, which represents not-for-profit long-term care providers.
Some measures call only for nursing homes to have a policy in place (for example, making sure the same staff serve residents every week), not to actually perform the tasks that the policy calls for, he noted.
State officials say it was important to start with a program that the industry would accept and that would not penalize large numbers of nursing homes. “Our plan is to up the ante” over time, said Kantor-Burman of the aging department. “After guidance, technical assistance, and engaging consumers on these issues for a year or two, we will expect more.”
Ultimately, the success or failure of Ohio’s program will depend on institutions like Welcome Nursing Home in Oberlin, a 102-bed facility operated by the same family since 1945. Jill Herron, the administrator, said her facility will meet 18 out of 20 standards set by the state, but she has questions about how well those requirements really reflect quality care.
Take the standard specifying that at least 50 percent of Medicaid-certified beds be in private rooms. That is impossible for the Welcome home, which has only six rooms of this type.
“Private rooms may be essential for market choice – people may want them and like them — but I don’t think they’re essential for quality care,” Herron said. “The fact is, most people come to nursing homes because they have an underlying medical condition and quality is about how we deal with that, while taking care of the whole person.”
Irene DuRell, an 82-year-old former nurse, has lived at the Welcome home for the past year with a 90-something roommate who she calls “wonderful.” “I’m very blessed we can talk to each other and she lets me help her out and she helps me out,” she said.
Asked what she likes best about Welcome, DuRell said, “The people have been nice. I can’t complain. They’ve been real good about helping out when I needed it. And they listen to me.”
Another administrator, Shane Craycraft of Garden Manor Extended Care Center in Middleton, questioned the requirement that overhead paging systems be turned off or used only in emergencies.
“While I think most people would be fine if they never heard overhead paging again, it’s not really going to affect most of the people out there,” he said. “That’s what we should be looking for with this incentive system: things that really make an impact.”

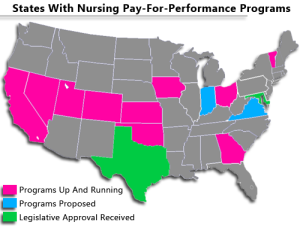
SOURCE: American Health Care Association, written communication, 2012; “State Adoption of Nursing Home Pay-for-Performance,” Medical Care Research and Review, June 2010