
The Growing Inequality in Life Expectancy Among Americans

(Moment/Getty Images)
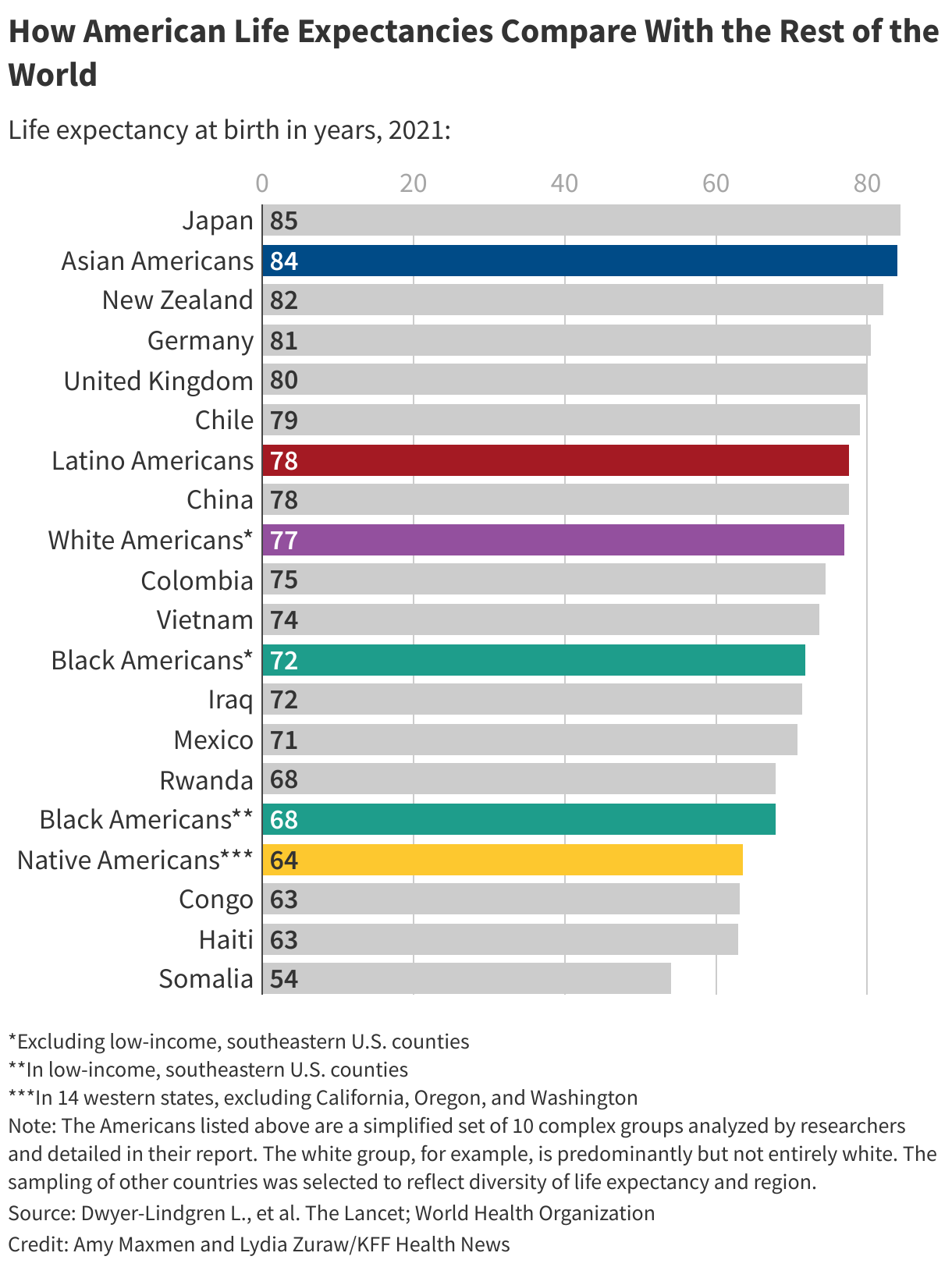
The life expectancy among Native Americans in the western United States has dropped below 64 years, close to life expectancies in the Democratic Republic of the Congo and Haiti. For many Asian Americans, it’s around 84 — on par with life expectancies in Japan and Switzerland.
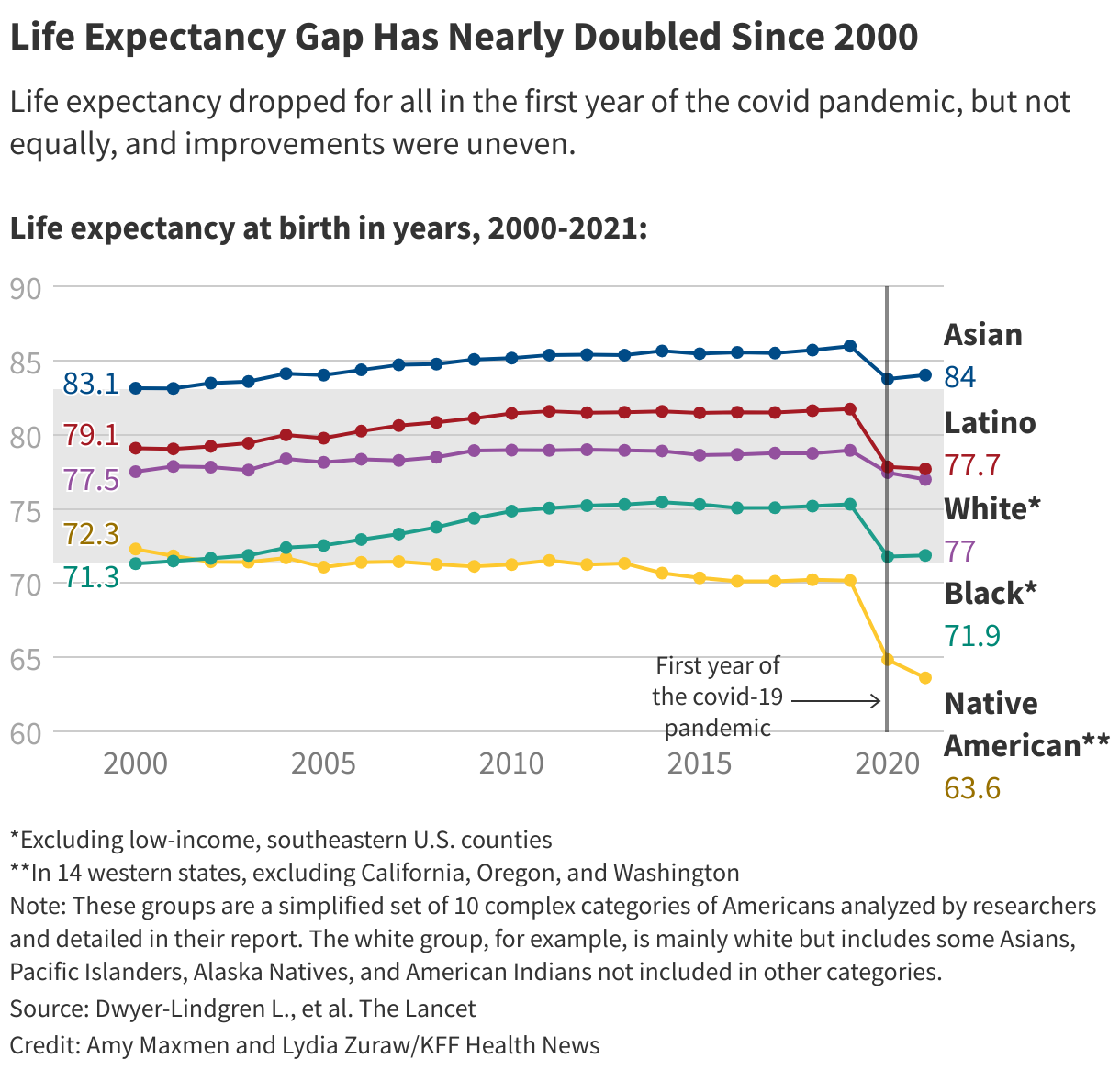
Americans’ health has long been unequal, but a new study shows that the disparity between the life expectancies of different populations has nearly doubled since 2000. “This is like comparing very different countries,” said Tom Bollyky, director of the global health program at the Council on Foreign Relations and an author of the study.
Called “Ten Americas,” the analysis published late last year in The Lancet found that “one’s life expectancy varies dramatically depending on where one lives, the economic conditions in that location, and one’s racial and ethnic identity.” The worsening health of specific populations is a key reason the country’s overall life expectancy — at 75 years for men and 80 for women — is the shortest among wealthy nations.
To deliver on pledges from the new Trump administration to make America healthy again, policymakers will need to fix problems undermining life expectancy across all populations.
“As long as we have these really severe disparities, we’re going to have this very low life expectancy,” said Kathleen Harris, a sociologist at the University of North Carolina. “It should not be that way for a country as rich as the U.S.”
Since 2000, the average life expectancy of many American Indians and Alaska Natives has been steadily shrinking. The same has been true since 2014 for Black people in low-income counties in the southeastern U.S.
“Some groups in the United States are facing a health crisis,” Bollyky said, “and we need to respond to that because it’s worsening.”
Heart disease, car fatalities, diabetes, covid-19, and other common causes of death are directly to blame. But research shows that the conditions of people’s lives, their behaviors, and their environments heavily influence why some populations are at higher risk than others.
Native Americans in the West — defined in the “Ten Americas” study as more than a dozen states excluding California, Washington, and Oregon — were among the poorest in the analysis, living in counties where a person’s annual income averages below about $20,000. Economists have shown that people with low incomes generally live shorter lives.
Studies have also linked the stress of poverty, trauma, and discrimination to detrimental coping behaviors like smoking and substance use disorders. And reservations often lack grocery stores and clean, piped water, which makes it hard to buy and cook healthy food.
About 1 in 5 Native Americans in the Southwest don’t have health insurance, according to a KFF report. Although the Indian Health Service provides coverage, the report says the program is weak due to chronic underfunding. This means people may delay or skip treatments for chronic illnesses. Postponed medical care contributed to the outsize toll of covid among Native Americans: About 1 of every 188 Navajo people died of the disease at the peak of the pandemic.
“The combination of limited access to health care and higher health risks has been devastating,” Bollyky said.
At the other end of the spectrum, the study’s category of Asian Americans maintained the longest life expectancies since 2000. As of 2021, it was 84 years.
Education may partly underlie the reasons certain groups live longer. “People with more education are more likely to seek out and adhere to health advice,” said Ali Mokdad, an epidemiologist at the Institute for Health Metrics and Evaluation at the University of Washington, and an author of the paper. Education also offers more opportunities for full-time jobs with health benefits. “Money allows you to take steps to take care of yourself,” Mokdad said.
The group with the highest incomes in most years of the analysis was predominantly composed of white people, followed by the mainly Asian group. The latter, however, maintained the highest rates of college graduation, by far. About half finished college, compared with fewer than a third of other populations.
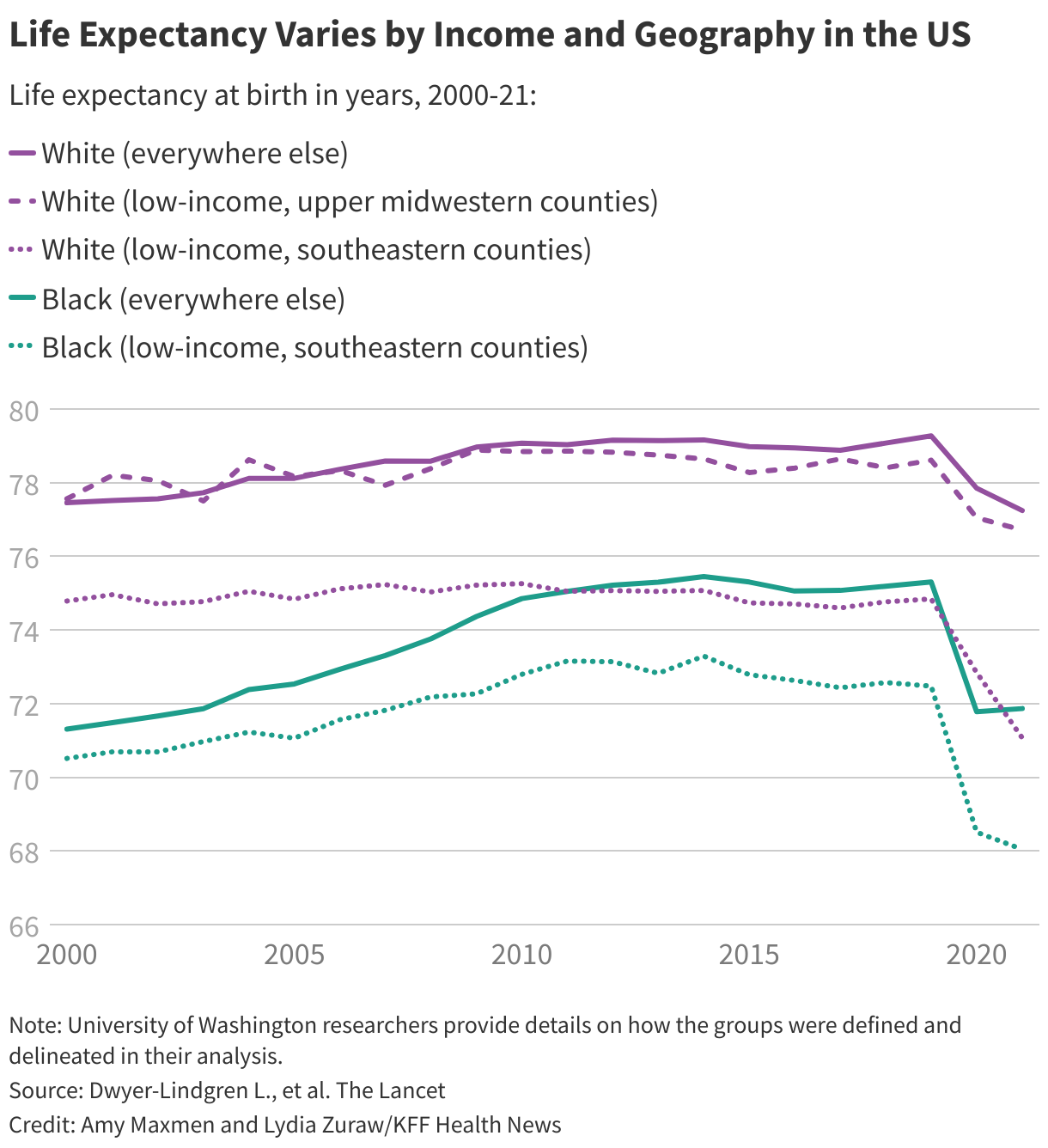
The study suggests that education partly accounts for differences among white people living in low-income counties, where the individual income averaged less than $32,363. Since 2000, white people in low-income counties in southeastern states — defined as those in Appalachia and the Lower Mississippi Valley — had far lower life expectancies than those in upper midwestern states including Montana, Nebraska, and Iowa. (The authors provide details on how the groups were defined and delineated in their report.)
Opioid use and HIV rates didn’t account for the disparity between these white, low-income groups, Bollyky said. But since 2010, more than 90% of white people in the northern group were high school graduates, compared with around 80% in the southeastern U.S.
The education effect didn’t hold true for Latino groups compared with others. Latinos saw lower rates of high school graduation than white people but lived longer on average. This long-standing trend recently changed among Latinos in the Southwest because of covid. Hispanic or Latino and Black people were nearly twice as likely to die from the disease.
On average, Black people in the U.S. have long experienced worse health than other races and ethnicities in the United States, except for Native Americans. But this analysis reveals a steady improvement in Black people’s life expectancy from 2000 to about 2012. During this period, the gap between Black and white life expectancies shrank.
This is true for all three groups of Black people in the analysis: Those in low-income counties in southeastern states like Mississippi, Louisiana, and Alabama; those in highly segregated and metropolitan counties, such as Queens, New York, and Wayne, Michigan, where many neighborhoods are almost entirely Black or entirely white; and Black people everywhere else.
Better drugs to treat high blood pressure and HIV help account for the improvements for many Americans between 2000 to 2010. And Black people, in particular, saw steep rises in high school graduation and gains in college education in that period.
However, progress stagnated for Black populations by 2016. Disparities in wealth grew. By 2021, Asian and many white Americans had the highest incomes in the study, living in counties with per capita incomes around $50,000. All three groups of Black people in the analysis remained below $30,000.
A wealth gap between Black and white people has historical roots, stretching back to the days of slavery, Jim Crow laws, and policies that prevented Black people from owning property in neighborhoods that are better served by public schools and other services. For Native Americans, a historical wealth gap can be traced to a near annihilation of the population and mass displacement in the 19th and 20th centuries.
Inequality has continued to rise for several reasons, such as a widening pay gap between predominantly white corporate leaders and low-wage workers, who are disproportionately people of color. And reporting from KFF Health News shows that decisions not to expand Medicaid have jeopardized the health of hundreds of thousands of people living in poverty.
Researchers have studied the potential health benefits of reparation payments to address historical injustices that led to racial wealth gaps. One new study estimates that such payments could reduce premature death among Black Americans by 29%.
Less controversial are interventions tailored to communities. Obesity often begins in childhood, for example, so policymakers could invest in after-school programs that give children a place to socialize, be active, and eat healthy food, Harris said. Such programs would need to be free for children whose parents can’t afford them and provide transportation.
But without policy changes that boost low wages, decrease medical costs, put safe housing and strong public education within reach, and ensure access to reproductive health care including abortion, Harris said, the country’s overall life expectancy may grow worse.
“If the federal government is really interested in America’s health,” she said, “they could grade states on their health metrics and give them incentives to improve.”


