
AURORA, Colo. — As Britney Taylor toured the Mama Bird Maternity Wellness Spa during its grand opening this spring, she reflected on the birth of her first child: a confusing and lonely experience that resulted in an unplanned cesarean section and an extended period of postpartum depression.
But here in this city abutting Denver, local families and smiling doulas wandered amid a bright space resonating with upbeat music where primarily women of color can get massages, meet with birth professionals and support groups, and attend classes on breastfeeding, childbirth, and infant care.
“This is perfect,” Taylor said. Her next birth, she said, “will be completely different.”
About 12 miles away in northeastern Denver, staff members at the Families Forward Resource Center were readying a room where families that might have a hard time getting to the doctor will be able to easily meet with clinical staff about their medical questions. They also were preparing to hire a doula trainer to help increase the local number of birthing support workers of color.
A major goal of both organizations is to reduce a significant health disparity in Colorado: Black, Hispanic, and American Indian/Alaska Native babies die at higher rates than white and Asian/Pacific Islander babies.
“Separated out by race/ethnicity, our disparities are persistent and are quite stark,” said Dr. Sunah Susan Hwang, a neonatologist with the University of Colorado School of Medicine.
By several measures, including infant mortality, Colorado is considered one of the healthiest states. For every 1,000 live births, fewer than five babies die before reaching their first birthday, putting Colorado among about 15 states that have met a threshold well ahead of a national 2030 target.
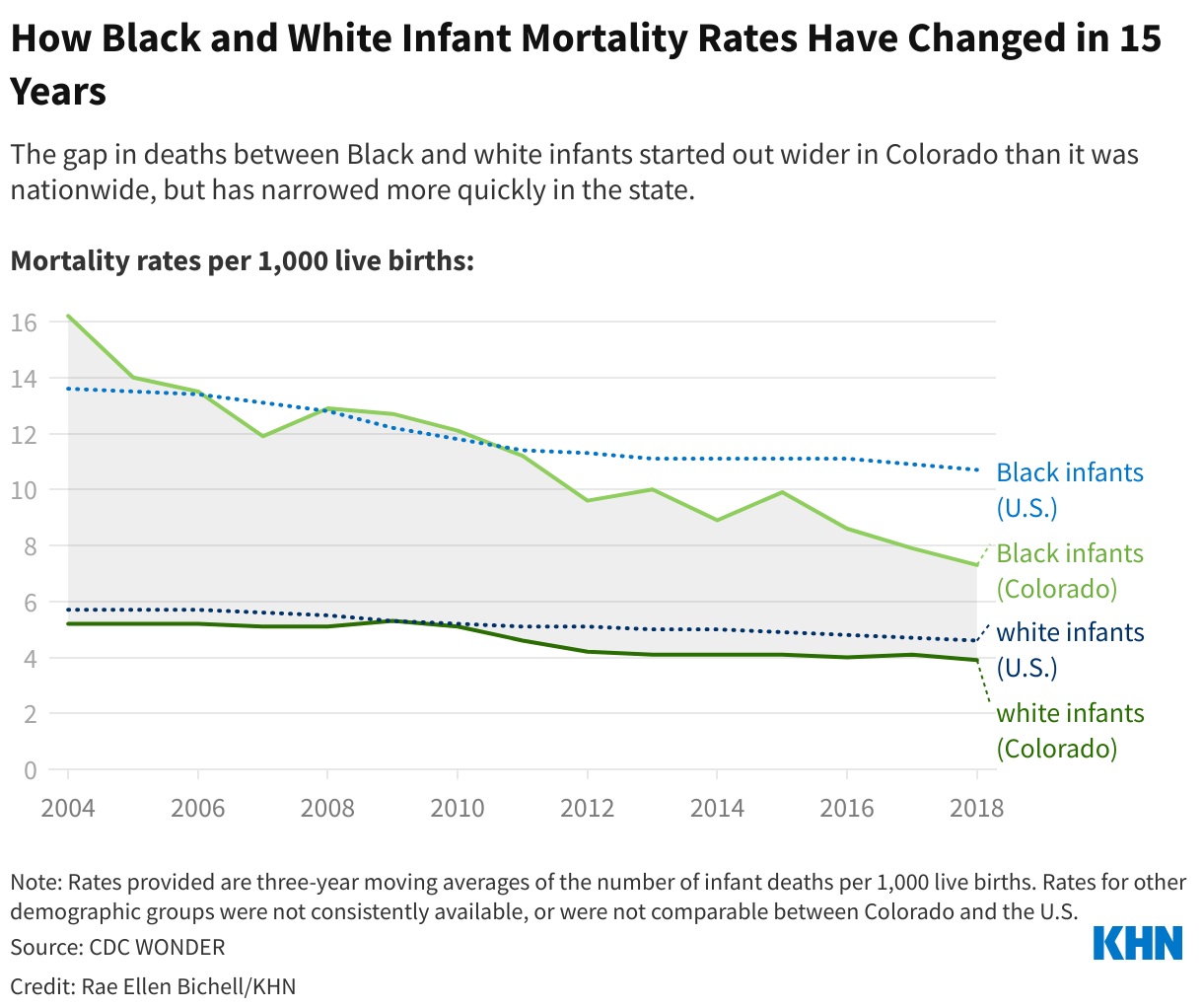
Centers for Disease Control and Prevention data for 2003 through 2019, the largest range for which comparable data is available, shows that the gap between non-Hispanic Black and non-Hispanic white infant mortality rates has narrowed more quickly in Colorado than nationally. The Colorado gap started out wider than the national gap but is now narrower.
But according to state health department data, only Asian/Pacific Islander and non-Hispanic white babies have reached the 2030 goal. And despite a dramatic drop in mortality among Black babies in the past 20 years, their mortality rate, at about 10 deaths per 1,000 live births in 2020, remains far higher than the state average. Hispanic babies, meanwhile, are still dying at about the same rate as 20 years ago, with more than six deaths per 1,000 live births. (Data for American Indian/Alaska Native babies was not consistently available because the numbers were too small to yield meaningful rates.)
If Black and Hispanic infants had the same infant mortality rate as non-Hispanic white infants in the state, about 200 babies would have been spared from 2018 to 2020 alone, according to a KHN data analysis.
One major reason babies die is that they are born too early. According to March of Dimes data, Colorado was among 22 states where a preterm birth disparity between the best-faring demographic and the rest of the population has worsened in the past five years. The state health department is clear on one big factor: racism.
“We know that racism and structural racism is one of the root causes that can be contributing to that chronic stress in people's lives that can contribute to prematurity, which can then lead to infant mortality,” said Mandy Bakulski, maternal and infant wellness section manager for the state health department.
Infant mortality is just one health measure that disproportionately affects Black, Hispanic, and American Indian/Alaska Native Coloradans: Compared with other Coloradans, they are more likely to die of kidney disease, diabetes, covid-19, car crashes, and other maladies, according to the state health department.
Bakulski said that in recent years state health officials have “flipped” their approach in reaction to community feedback on the state’s infant mortality gaps, and a multistate project that studied a wide range of possible interventions. Bakulski’s team said the combination led them to conclude that “getting money in the pockets of people was a way that we could be improving health outcomes.”
So the department has been pushing the benefit of child tax credits that allow families to keep more of their income and is gearing up to promote a law that, starting in 2024, will give many Colorado parents three months of partially paid leave to care for a new child.
According to the March of Dimes — which tracks state efforts to reduce infant mortality and preterm birth — Colorado has achieved four out of six policy measures thought to improve maternal and infant health, which are closely intertwined. Most important, it expanded Medicaid in 2013, which researchers say helps to lower infant mortality, though it’s unclear whether it has helped narrow racial gaps.
“We give Colorado a ‘B.’ That is much better than a lot of states — certainly better than the states that are surrounding Colorado,” said Edward Bray, senior director of state affairs for March of Dimes. But there is “room for improvement.”
One imminent change the organization expects will help: Colorado is in the process of temporarily extending Medicaid eligibility, so that more low-income women will have coverage for a year after they give birth, rather than the typical two months. That change is part of a bundle of laws passed last year that, among other things, elevated medical mistreatment during the perinatal period to a civil rights issue reportable to the Colorado Civil Rights Commission.
However, advocates, researchers, and professionals who work with families of color say there is more the state can and should do. First, they say, create a workforce of culturally competent care providers, including doulas.
“Research has supported that doulas help with better outcomes in general for births, reduced preterm births, and reduced both maternal and infant mortality and morbidity,” said Bray, whose organization identified doula access as one of Colorado’s main policy shortcomings.
However, Anu Manchikanti Gómez, a health equity researcher at the University of California-Berkeley who studies interventions, including doula care, designed to improve birth outcomes, said other options could be pivotal too. While a doula plays an important role as a support person, a navigator, and an advocate, she said, the doula is “a very downstream solution. It's not really addressing the root of the problem.”
Gómez is interested in concrete interventions like no-strings-attached cash transfers to expecting families. In Canada, researchers found that when Indigenous women who were pregnant and poor received a cash benefit of about $60 a month, it helped families meet their needs and reduce stress, and babies were less likely to be born early or small.
Gómez is involved in a pilot study, the Abundant Birth Project, which gives a monthly cash supplement of about $1,000 to pregnant women in San Francisco who are Black or Pacific Islander. The goal is to relieve types of stress that can lead to preterm birth.
Grassroots groups, meanwhile, are minding the gaps in policy, acting as the problem-solvers in their communities while waiting for the policymakers to catch up.
For example, Birdie, the owner of Mama Bird Maternity Wellness Spa, is working with Colorado Access, one of the state’s Medicaid providers, to see if they can get doulas reimbursed for working with low-income families — one of the major gaps in Colorado identified by March of Dimes. In Aurora, where the maternity center is located, fewer than half of residents are white.
“We’re serving women of color,” said Birdie, who goes by one name. “Our measure of success is happy mom, happy baby.”
Nearby, Families Forward Resource Center has received federal funding to support women prone to high-risk pregnancies and to train professionals who can help with birth, breastfeeding, and postpartum care.

It's run by people who know firsthand what it is like to experience bias in health care, such as Joy Senyah, whose son was born early and died within two days. Her doctors ignored her heavy bleeding before birth and, after an emergency C-section, they found he had been detached from the placenta for hours.
“Every time I asked, it was dismissed: ‘Ma’am, you’re fine,’” said Senyah, who was alone during the birth and covered by Medicaid. “When I look in hindsight at the situation, of course, I'm like, ‘Yeah, you should have known. You should have raised hell.’”
She’s now the outreach specialist for the resource center, working with her colleagues toward the goal that babies of color will have the same chance at surviving their first year as other babies. A big part of that is figuring out how to support families and provide them with access to breastfeeding consultants, birth workers, and medical professionals who understand their clients — and are ready to help raise hell if necessary.
Methodology
KHN analyzed Linked Birth/Infant Death Records data from the Centers for Disease Control and Prevention’s WONDER database for the years 2003-2006 and 2017-2019. To characterize how the Black-white infant mortality rate gaps changed over that period at the national level and in Colorado, three-year averages were calculated for each demographic group and the resulting rate for the 2017-2019 time frame was compared with the 2003-2005 rate.
For state specifics, data from 2000 through 2020 was provided by the Colorado Department of Health and Environment. Three-year moving averages were calculated across that period for each demographic group.
To calculate excess deaths from 2018 to 2020, the three-year average infant mortality rate for white babies was subtracted from the three-year average infant mortality rate for Black babies. The resulting excess infant mortality rate was multiplied by the three-year sum of live births over that period and divided by 1,000.
Latoya Hill, a senior policy analyst with KFF’s Racial Equity and Health Policy Program, identified appropriate analysis methods, and Tessa Crume, an associate professor of epidemiology at the Colorado School of Public Health, confirmed the conclusions.



