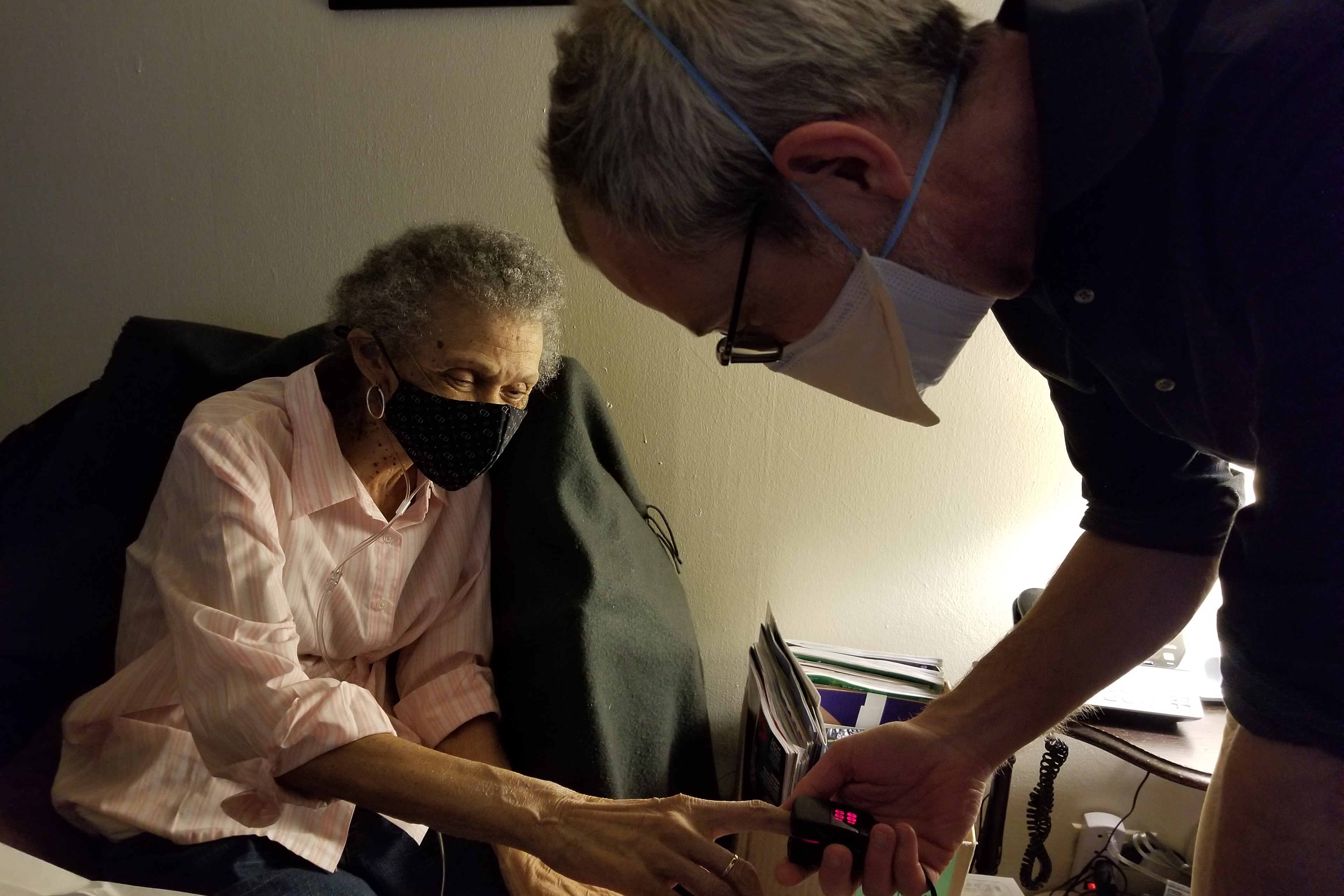
Carolyn Dickens, 76, was sitting at her dining room table, struggling to catch her breath as her physician looked on with concern.
“What’s going on with your breathing?” asked Peter Gliatto, director of Mount Sinai’s Visiting Doctors Program.
“I don’t know,” she answered, so softly it was hard to hear. “Going from here to the bathroom or the door, I get really winded. I don’t know when it’s going to be my last breath.”
Dickens, a lung cancer survivor, lives in central Harlem, barely getting by. She has serious lung disease and high blood pressure and suffers regular fainting spells. In the past year, she’s fallen several times and dropped to 85 pounds, a dangerously low weight.
And she lives alone, without any help — a highly perilous situation.
Across the country, about 2 million adults 65 and older are completely or mostly homebound, while an additional 5.5 million seniors can get out only with significant difficulty or assistance. This is almost surely an undercount, since the data is from more than a dozen years ago.
It’s a population whose numbers far exceed those living in nursing homes — about 1.2 million — and yet it receives much less attention from policymakers, legislators, and academics who study aging.
Consider some eye-opening statistics about completely homebound seniors from a study published in 2020 in JAMA Internal Medicine: Nearly 40% have five or more chronic medical conditions, such as heart or lung disease. Almost 30% are believed to have “probable dementia.” Seventy-seven percent have difficulty with at least one daily task such as bathing or dressing.
Almost 40% live by themselves.
That “on my own” status magnifies these individuals’ already considerable vulnerability, something that became acutely obvious during the covid-19 outbreak, when the number of sick and disabled seniors confined to their homes doubled.
“People who are homebound, like other individuals who are seriously ill, rely on other people for so much,” said Katherine Ornstein, director of the Center for Equity in Aging at the Johns Hopkins School of Nursing. “If they don’t have someone there with them, they’re at risk of not having food, not having access to health care, not living in a safe environment.”
Research has shown that older homebound adults are less likely to receive regular primary care than other seniors. They’re also more likely to end up in the hospital with medical crises that might have been prevented if someone had been checking on them.
To better understand the experiences of these seniors, I accompanied Gliatto on some home visits in New York City. Mount Sinai’s Visiting Doctors Program, established in 1995, is one of the oldest in the nation. Only 12% of older U.S. adults who rarely or never leave home have access to this kind of home-based primary care.
Gliatto and his staff — seven part-time doctors, three nurse practitioners, two nurses, two social workers, and three administrative staffers — serve about 1,000 patients in Manhattan each year.
These patients have complicated needs and require high levels of assistance. In recent years, Gliatto has had to cut staff as Mount Sinai has reduced its financial contribution to the program. It doesn’t turn a profit, because reimbursement for services is low and expenses are high.
First, Gliatto stopped in to see Sandra Pettway, 79, who never married or had children and has lived by herself in a two-bedroom Harlem apartment for 30 years.
Pettway has severe spinal problems and back pain, as well as Type 2 diabetes and depression. She has difficulty moving around and rarely leaves her apartment. “Since the pandemic, it’s been awfully lonely,” she told me.
When I asked who checks in on her, Pettway mentioned her next-door neighbor. There’s no one else she sees regularly.
Pettway told the doctor she was increasingly apprehensive about an upcoming spinal surgery. He reassured her that Medicare would cover in-home nursing care, aides, and physical therapy services.
“Someone will be with you, at least for six weeks,” he said. Left unsaid: Afterward, she would be on her own. (The surgery in April went well, Gliatto reported later.)
The doctor listened carefully as Pettway talked about her memory lapses.
“I can remember when I was a year old, but I can’t remember 10 minutes ago,” she said. He told her that he thought she was managing well but that he would arrange testing if there was further evidence of cognitive decline. For now, he said, he’s not particularly worried about her ability to manage on her own.


Several blocks away, Gliatto visited Dickens, who has lived in her one-bedroom Harlem apartment for 31 years. Dickens told me she hasn’t seen other people regularly since her sister, who used to help her out, had a stroke. Most of the neighbors she knew well have died. Her only other close relative is a niece in the Bronx whom she sees about once a month.
Dickens worked with special-education students for decades in New York City’s public schools. Now she lives on a small pension and Social Security — too much to qualify for Medicaid. (Medicaid, the program for low-income people, will pay for aides in the home. Medicare, which covers people over age 65, does not.) Like Pettway, she has only a small fixed income, so she can’t afford in-home help.
Every Friday, God’s Love We Deliver, an organization that prepares medically tailored meals for sick people, delivers a week’s worth of frozen breakfasts and dinners that Dickens reheats in the microwave. She almost never goes out. When she has energy, she tries to do a bit of cleaning.
Without the ongoing attention from Gliatto, Dickens doesn’t know what she’d do. “Having to get up and go out, you know, putting on your clothes, it’s a task,” she said. “And I have the fear of falling.”
The next day, Gliatto visited Marianne Gluck Morrison, 73, a former survey researcher for New York City’s personnel department, in her cluttered Greenwich Village apartment. Morrison, who doesn’t have any siblings or children, was widowed in 2010 and has lived alone since.
Morrison said she’d been feeling dizzy over the past few weeks, and Gliatto gave her a basic neurological exam, asking her to follow his fingers with her eyes and touch her fingers to her nose.
“I think your problem is with your ear, not your brain,” he told her, describing symptoms of vertigo.
Because she had severe wounds on her feet related to Type 2 diabetes, Morrison had been getting home health care for several weeks through Medicare. But those services — help from aides, nurses, and physical therapists — were due to expire in two weeks.
“I don’t know what I’ll do then, probably just spend a lot of time in bed,” Morrison told me. Among her other medical conditions: congestive heart failure, osteoarthritis, an irregular heartbeat, chronic kidney disease, and depression.
Morrison hasn’t left her apartment since November 2023, when she returned home after a hospitalization and several months at a rehabilitation center. Climbing the three steps that lead up into her apartment building is simply too hard.
“It’s hard to be by myself so much of the time. It’s lonely,” she told me. “I would love to have people see me in the house. But at this point, because of the clutter, I can’t do it.”
When I asked Morrison who she feels she can count on, she listed Gliatto and a mental health therapist from Henry Street Settlement, a social services organization. She has one close friend she speaks with on the phone most nights.
“The problem is I’ve lost eight to nine friends in the last 15 years,” she said, sighing heavily. “They’ve died or moved away.”
Bruce Leff, director of the Center for Transformative Geriatric Research at the Johns Hopkins School of Medicine, is a leading advocate of home-based medical care. “It’s kind of amazing how people find ways to get by,” he said when I asked him about homebound older adults who live alone. “There’s a significant degree of frailty and vulnerability, but there is also substantial resilience.”
With the rapid expansion of the aging population in the years ahead, Leff is convinced that more kinds of care will move into the home, everything from rehab services to palliative care to hospital-level services.
“It will simply be impossible to build enough hospitals and health facilities to meet the demand from an aging population,” he said.
But that will be challenging for homebound older adults who are on their own. Without on-site family caregivers, there may be no one around to help manage this home-based care.



