In Fierce Debate, Democratic Candidates Expand Health Agenda Arguments
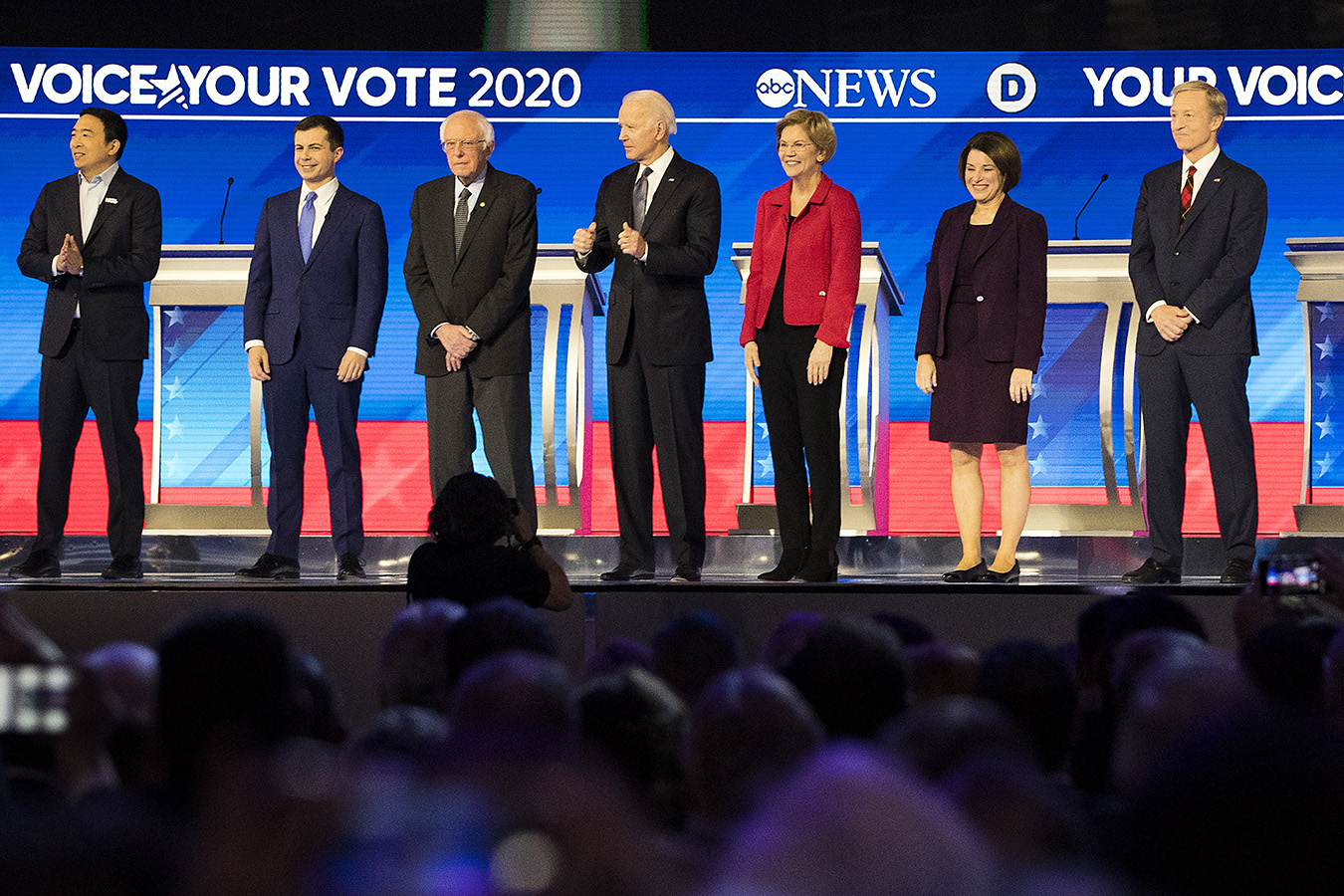
Democratic presidential candidates (left to right) Andrew Yang, South Bend, Ind., Mayor Pete Buttigieg, Sen. Bernie Sanders (I-Vt.), former Vice President Joe Biden, Sen. Elizabeth Warren (D-Mass.), Sen. Amy Klobuchar (D-Minn.) and Tom Steyer take the stage before the Democratic presidential primary debate at Saint Anselm College in Manchester, New Hampshire. (Adam Glanzman/Getty Images)
Democratic presidential candidates faced off on the debate stage for the eighth time this campaign season. Meeting in Manchester, N.H., they returned to now familiar health care themes — “Medicare for All” versus a public option, the cost of prescription drugs and other key areas they say are ripe for change.
Once again, candidates sparred over the cost of the single-payer health reform bill promoted by Vermont Sen. Bernie Sanders. Former Vice President Joe Biden argued it would necessarily raise taxes, pointing to its estimated $32 trillion price-tag (a number supported by independent economist estimates). Sanders noted that over the next decade, the nation is projected to end up spending more than $50 trillion on health care. (That’s also borne out by evidence.)
Sen. Elizabeth Warren of Massachusetts and Sen. Amy Klobuchar of Minnesota also dove into issues related to abortion rights. Warren touted the statistic that three out of four Americans believe that Roe v. Wade should be the law. This is pretty accurate — a recent Kaiser Family Foundation poll found that 69% of Americans do not want Roe v. Wade overturned. And Klobuchar again talked about how there is overwhelming support for Planned Parenthood. We previously checked this claim.
The candidates also discussed the opioid epidemic and the shortage of substance abuse treatment beds — in New Hampshire and nationwide.
Here are some highlights and related fact checks:
You sent out a tweet just a few years ago you said ‘henceforth, forewith you are for Medicare for all for the ages.’
Sen. Amy Klobuchar, Feb. 7, 2020
The truth is I have been consistent throughout in my position on health care for every American.
Former South Bend Mayor Pete Buttigieg, Feb. 7, 2020
Klobuchar and Buttigieg, the former mayor of South Bend, Ind., sparred over his record of support for Medicare for All, the single-payer health care bill Sanders backs. Klobuchar noted that Buttigieg previously tweeted in favor of the bill and has since changed his position. Buttigieg said he has been consistent on supporting an approach that would bring health care to all Americans.
Klobuchar’s point — that Buttigieg has at least expressed support for the specific bill, and no longer does — is supported by evidence.
The tweet was posted on Feb. 18, 2018. Buttigieg wrote, “I, Pete Buttigieg, politician, do henceforth and forthwith declare, most affirmatively and indubitably, unto the ages, that I do favor Medicare for All, as I do favor any measure that would help get all Americans covered.”
Since then, Buttigieg has narrowed his stance — backing “Medicare for all who want it,” a plan he argues would also achieve universal coverage, by letting people opt into a public health plan, and offering more generous subsidies for those who purchase private insurance. (Proponents of single-payer are skeptical it would succeed.)
To be fair, even Buttigieg’s 2018 statement includes an important qualifier — he’s not tied to the plan. He favors Medicare for All, he says, as he does “any measure that would help get all Americans covered.” If you agree that his current plan would also achieve universal health care, there’s an argument that he has been consistent.
—Shefali Luthra
It would cost more than the entire federal budget that we spend now.
Former Vice President Joe Biden, Feb. 7, 2020
This is in reference to Medicare for All. We contacted Biden’s campaign, who directed us to the 2018 federal budget — $4.1 trillion — compared to the estimated $32 trillion price tag of Sanders’ single-payer proposal. But there’s a problem: That latter number is an estimate of the cost for 10 years. So putting one year of the budget against a decade of health spending is comparing apples and oranges.
And converting one year’s budget to a decade-long forecast is an economically complex proposition — it’s not so simple as just multiplying by 10.
We also ran this claim by an independent expert, who crunched the $32 trillion estimate. Linda Blumberg, an institute fellow at the Urban Institute, told us Biden’s comparison is “an exaggeration” and “overstatement.”
Certainly, she said, Medicare for All would be “a bigger increase to the federal budget than we’ve ever experienced” — more than a 70% increase, compared to the CBO’s 10-year budget estimate.
“This is an enormous increase, but it wouldn’t double” the budget, she said.
—Shefali Luthra
The health care industry makes $100 billion in profit.
Sen. Bernie Sanders, Feb. 7, 2020
This is a favorite talking point from Sanders. We double-checked the math during the last debate. It holds up — and is probably an underestimate.
The figure is derived by adding the “net revenues” as reported by the companies for 10 pharmaceutical companies and 10 companies that work in health insurance. Multiple independent economists reviewed the methodology with, and affirmed that it’s sound. In fact, the total “net revenue” — or profit — is actually around $101 billion.
The talking point doesn’t include health care’s biggest earners, though: hospitals and health systems. When you factor them in, experts previously told us, the level of profit in our system will grow significantly larger.
—Shefali Luthra
30,000 Americans a year die waiting for health care because of the cost.
Sen. Bernie Sanders, Feb. 7, 2020
The way Sanders uses this number is problematic and oversimplifies the research. When we previously fact-checked this claim, we rated it Half True.
It appears that the number comes from Physicians for a National Health Program, which cited the Oregon Health Insurance Experiment, a study that assigned by lottery some participants to Medicaid and the others remained without insurance. A year into the experiment, researchers found that the death rate differed by 0.13 percentage points between those who were on Medicaid and those who were not — though this difference was not statistically significant. If you extrapolate this number to the number of Americans who are uninsured — about 27 million — then you do get close to a figure of about 30,000 people.
However, experts said that since the difference was not statistically significant it shouldn’t be extrapolated so broadly, and it’s possible that Sanders’ number is too high. Other research does show that there is a connection between being uninsured and higher likelihood of mortality. Thousands of Americans die waiting for health care every year, but this number relies on imprecise math.
—Victoria Knight
36 million Americans last year couldn’t afford to fill a prescription, including those with insurance.
Sen. Elizabeth Warren, Feb. 7, 2020
This is true. If anything, it falls a little short.
The data comes from an estimate by the Commonwealth Fund, a health care research and advocacy group. Researchers found that in 2018, 37 million non-elderly Americans — about 1 in 5 people — skipped a prescription because they couldn’t afford it. Some of those people had coverage. Others were “underinsured.” That means they had insurance, but it wasn’t enough to safeguard them from large medical bills.
Other data suggests it’s potentially even worse. A November poll from West Health and Gallup estimated that 58 million Americans experienced what they called “medication insecurity” in the past 12 months.
—Shefali Luthra
How about we start with what a president can do — I love saying this — all by herself? On day one I will defend the Affordable Care Act and use march-in orders to reduce the costs of commonly used prescription drugs like insulin and HIV/AIDS drugs and EpiPens.
Sen. Elizabeth Warren, Feb. 7, 2020
On the campaign trail, Warren has often mentioned that she would use the power of the executive office to reduce prescription drug prices for drugs such as HIV medication and EpiPens. We checked it, and it is true that the president has these executive powers.
Warren has in her “Medicare for All” transition plan a pledge that she would use two legal mechanisms to achieve this goal — “compulsory licensing” and march-in rights. Compulsory licensing means the government will take over a patent if a drug’s prices are too high and create competition. There is precedent for this approach, it was done in the 1960s for cheap generic drugs and in 2001 for Ciprofloxacin during the anthrax scare. Experts said this likely couldn’t be applied to all drugs but could work for insulin and EpiPens.
March-in rights are when the government “marches in” during a public health crisis because a drug isn’t available. But, it only works for drugs in which the government holds all of the patents, such as Truvada, the HIV prevention drug. However, this mechanism has never been employed and it’s unclear whether high prescription drug prices would qualify as a public health concern. Officials at the National Institutes of Health would also have to approve this measure, and it would face significant backlash from the pharmaceutical industry.
Warren is right that the laws are in place for her to reduce prescription drug prices without the power of Congress, but it’s likely it would be difficult.
—Victoria Knight