Errors in Deloitte-Run Medicaid Systems Can Cost Millions and Take Years To Fix

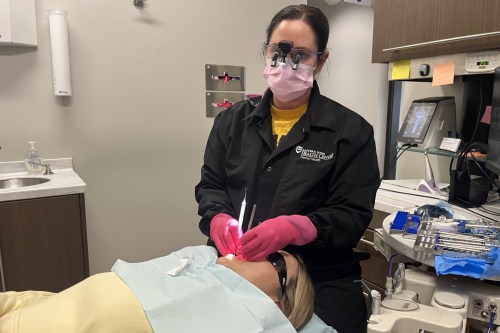
As states wait for Deloitte to make fixes in computer systems, Medicaid beneficiaries risk losing access to health care and food. (CFOTO/Future Publishing via Getty Images)
The computer systems run by the consulting giant Deloitte that millions of Americans rely on for Medicaid and other government benefits are prone to errors that can take years and hundreds of millions of dollars to update. While states wait for fixes from Deloitte, beneficiaries risk losing access to health care and food.
Changes needed to fix Deloitte-run eligibility systems often pile on costs to the government that are much higher than the original contracts, which can slow the process of fixing errors.
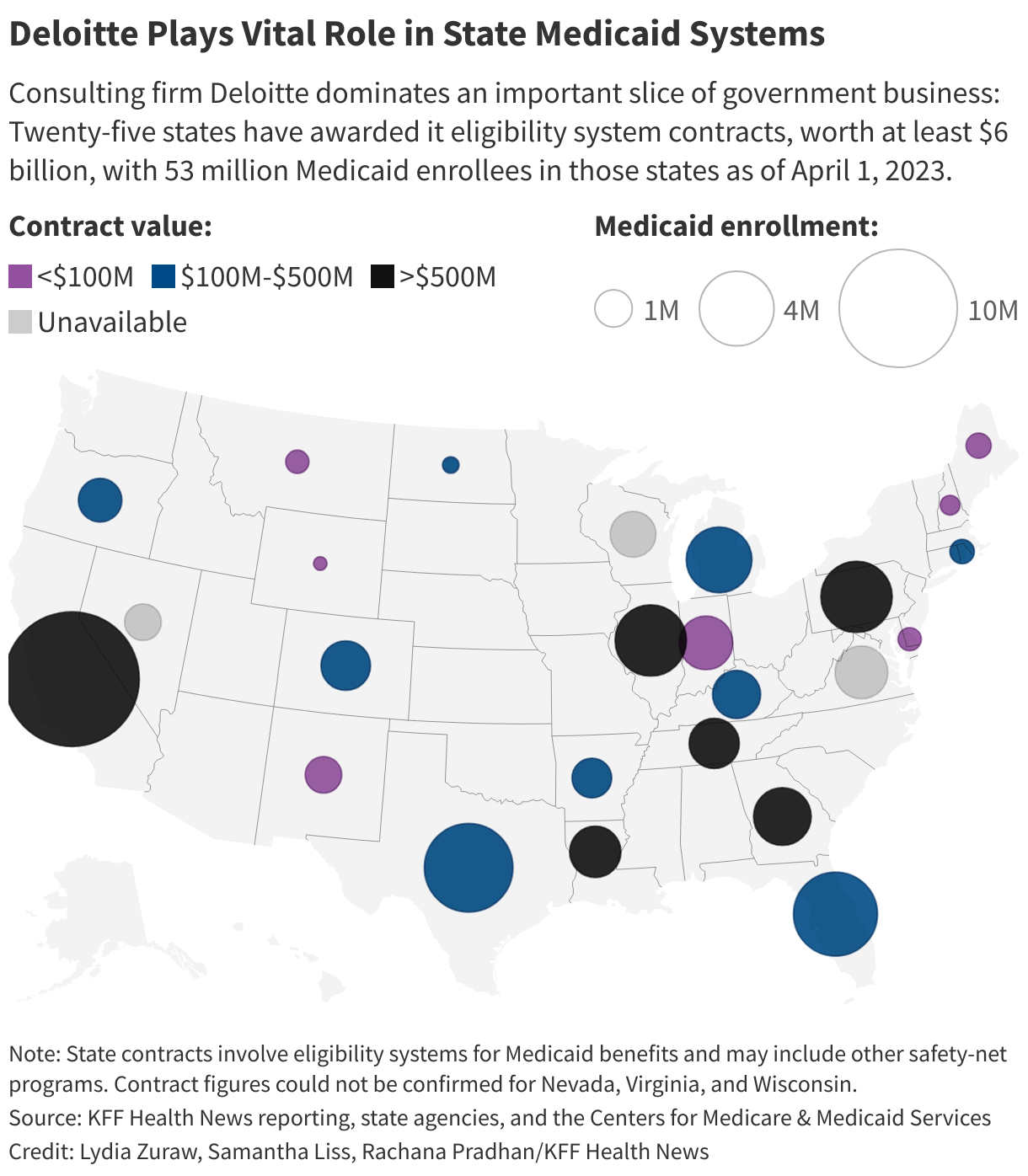
It has become a big problem across the country. Twenty-five states have awarded Deloitte contracts for eligibility systems, giving the company a stronghold in a lucrative segment of the government benefits business. The agreements, in which the company commits to design, develop, implement, or operate state-owned systems, are worth at least $6 billion, dwarfing any of its competitors, a KFF Health News investigation found.
Problems and delays can extend beyond Medicaid — which provides health coverage to roughly 75 million low-income people — because some state systems assess eligibility for other safety-net programs. Whether a person gets the benefits they are entitled to depends on what the computer says.
There is no automatic switch to stop errors in the system, said Elizabeth Edwards, a senior attorney with the National Health Law Program, a nonprofit that advocates for people with low incomes and medically underserved populations. The group in January filed a complaint urging the Federal Trade Commission to investigate Deloitte, alleging “ongoing and nationwide” errors and “unfair and deceptive trade practices.”
“People will go without care,” Edwards said, and until there’s a fix or a workaround, “you will continue to have the harm over and over again.”
Kenneth Smith, a Deloitte executive who leads its national human services division, previously told KFF Health News that Medicaid eligibility technology is state-owned and agencies “direct their operation” and “make decisions about the policies and processes that they implement.” Smith has called the legal nonprofit’s allegations “without merit.”
States set aside millions of dollars to cover the cost of changes, but systems may require fixes beyond the agreed-upon work. The number of hours or updates is capped each year, so states are left to prioritize certain fixes over others. And even though Deloitte isn’t reinventing the wheel for each eligibility system it builds or runs, the company addresses problems state by state rather than patching through fixes for systems across states, Smith said — a change request in one state “likely has absolutely nothing to do with another state.”
“Because of the custom nature of these systems, it’s never quite that simplistic as, ‘Hey, a particular issue that’s arisen in state of A is directly applicable to state of B,’” Smith said.
Speaking generally, Smith said, “I’m unaware of any circumstance in which a client has needed to get something done that we haven’t found a way to get it done.”
The work is lucrative for Deloitte, which reported global revenue of $65 billion in fiscal year 2023.
Deloitte’s estimates show that 35 change requests for Georgia’s eligibility system in 2023 would take more than 104,000 hours of work, according to a list of change requests that KFF Health News obtained in response to a public records request. That’s the equivalent of 50 years of work, if someone worked 52 weeks a year at 40 hours a week.
“System changes were made to align with changing federal and state policies, as well as to meet evolving business needs," said Ellen Brown, a spokesperson for the Georgia Department of Human Services. Brown earlier said changes also were made to “improve functionality.”
The federal government — that is, its taxpayers — covers 90% of states’ costs to develop and implement state Medicaid eligibility systems and pays 75% of ongoing maintenance and operations expenses, according to federal regulations.
Eligibility systems for years have posed problems for states because of the dynamic between contractors and government officials, said Matt Salo, CEO of consulting firm Salo Health Strategies. The companies hold the expertise “and, quite frankly, they’re kind of running circles around the state capacity,” said Salo, a former executive director of the National Association of Medicaid Directors.
“For decades all I’ve heard from states in this arena is: We know that when we go out to contract it’s going to cost us a lot of money and it is going to run over, it is going to deliver years late, it is going to deliver millions if not hundreds of millions of dollars over budget,” Salo said, and “by the time it’s delivered, our needs have changed and so it’s just this constant process of change orders and going back and fixing.”
Going to Court in Florida
Two advocacy groups last August sued Florida in federal court, alleging tens of thousands of people were losing coverage without proper warning. And Florida’s eligibility system was cutting off Medicaid coverage for some moms after giving birth, William Roberts, a state employee who reviews Medicaid eligibility decisions, testified when the case went to trial in July.
Florida previously gave moms two months of Medicaid coverage after giving birth. Federal regulators in 2022 approved Florida’s proposal to grant Medicaid benefits for 12 months. But in April 2023 state officials discovered a “glitch,” Roberts said, and “the system had reverted back to only giving mothers two months instead of giving them the 12 months that they were entitled to.”
What became clear in the testimony is that the state and Deloitte take different views on what constitutes a “defect” in a Deloitte-run system. Deloitte said it would fix defects without billing any additional hours for the work. Although Deloitte is not a named defendant in the lawsuit, the company was called to testify about its role in operating Florida’s eligibility system.
Harikumar Kallumkal, a Deloitte managing director who oversees the Florida system, initially testified that, in this case, there was no problem and “the computer system was providing 12 months” of postpartum coverage.
Then Kallumkal said, “Even in this case, I do not believe it was a defect.” Even so, “we did fix that.” And for the fix, he said, Deloitte “did not charge” the state.
Rather, a separate defect may have resulted in coverage losses for mothers after childbirth, Kallumkal testified.
Some historical data “required to determine postpartum coverage” was not loading into the system, Kallumkal said. “I don’t know how many cases it impacted,” he said, but Deloitte fixed the problem.
The courtroom revelation confirmed what Florida advocates already knew: an eligibility system issue prevented some of the state’s most vulnerable from getting care. Florida denied allegations that it terminated Medicaid coverage without providing adequate notice. The case is ongoing.
When Michigan resumed regular Medicaid eligibility checks following the covid-19 pandemic, advocates saw a concerning trend.
The computer system routinely fails to recognize when certain adults with disabilities should receive Medicaid benefits, said Dawn Calnen, executive director of The Arc of Oakland County, which provides support for those with intellectual and developmental disabilities.
Often a person who qualifies for Medicaid initially for one reason could remain eligible even when life circumstances change. Calnen said there’s no question that the people her group assisted are still eligible, just in a different way than during the pandemic.
The problem is frequent enough that Calnen’s group felt compelled to notify others. “We kind of shout it from the rooftop for people: Know that this is going to happen.”
When asked about the problem, Chelsea Wuth, a spokesperson for Michigan’s Department of Health and Human Services, said there were “no issues” with the system. Deloitte operates Michigan’s eligibility system. The company said it does not comment on state-specific issues.
Tennessee hired Deloitte in 2016 to build an eligibility system after the state canceled a contract with Northrop Grumman due to chronic delays. Deloitte didn’t create the Tennessee system, known as TEDS, from scratch. It built on components from Georgia’s system, according to a legal declaration and a deposition of Kimberly Hagan, Tennessee Medicaid’s director of member services, that were part of a class-action lawsuit that Medicaid beneficiaries filed against the state in 2020.
The lawsuit, which is ongoing and does not name Deloitte as a defendant, seeks to order Tennessee to restore coverage under its Medicaid program, known as TennCare, for those who wrongly lost it. Hagan, in a court filing, said many problems “reflect some unforeseen flaws or gaps” with the Tennessee eligibility system and “some design errors.”
A federal judge on Aug. 26 sided with the Medicaid beneficiaries, ruling that Tennessee violated federal law and the U.S. Constitution. “Poor, disabled, and otherwise disadvantaged Tennesseans should not require luck, perseverance, or zealous lawyering to receive healthcare benefits they are entitled to under the law,” wrote U.S. District Court Judge Waverly D. Crenshaw Jr., adding, “TEDS is flawed, and TennCare knows that it is flawed.”
Tennessee Medicaid spokesperson Amy Lawrence said the state is “determining what our next steps will be.”
Tennessee’s $823 million contract with Deloitte shows that the budget for changes outside the contract’s original scope increased by hundreds of millions of dollars. Deloitte’s maximum compensation for such change orders rose to $417 million under a 2023 contract amendment, up from $103.6 million four years earlier.
Lawrence said state officials “do not and would not pay to fix vendor errors.” Lawrence attributed the cost increases to “system modernization” in “an effort to enhance our citizens’ interactions with the state Medicaid program.” Additional funding was also needed to comply with new federal requirements related to the covid-19 pandemic, she said.
Waiting on Fixes
States sometimes wait so long for Deloitte’s fixes that the staffers who worked on the problems don’t see the results. Jamie Perkins was responsible for making letters easier for Colorado Medicaid enrollees to understand. The letters are generated by Colorado’s Deloitte-run eligibility system. State audits have found that the notices confuse enrollees and contain errors. Perkins said she left her job in 2021, frustrated that many of her fixes hadn’t been implemented.
“It feels like a really perverse reward system, frankly, for Deloitte,” Perkins said. “When Deloitte is themselves making a problem that did not originate with the department, the department is still paying them to fix those problems.”
The state’s contract with Deloitte now outlines “protocols to address issues that are the result of the contractor,” said Trish Grodzicki, a spokesperson for Colorado’s Medicaid agency. As of June 30, Colorado “has made substantial improvements” and a “majority of the letters have been rewritten” and updated in the system, she said.
Deloitte spokesperson Karen Walsh said “a change request can represent a number of different things,” including when states make policy decisions that would warrant system updates. Smith said Deloitte views change requests and system issues, or defects, as different things.
“We have a responsibility when there’s a system issue to fix that,” Walsh said. “We don’t get a change request to fix an issue.”
Yet in Kentucky and other places, states have submitted change orders to resolve issues. Government officials and Deloitte sometimes negotiate fixes for months before they’re implemented.
Kentucky resident Beverly Likens lost Medicaid coverage in June 2023 partly due to an error with the state’s Deloitte-run system. State health officials told a legal aid group in September 2023 that a “change order has been submitted” to fix the glitch, which blocked her new coverage application from getting through online.

Likens, with the help of a lawyer, had her Medicaid benefits quickly reinstated, but that was far from the end of the saga. The problem that caused her benefits to lapse was resolved in April — 10 months later — when Kentucky implemented the first phase of a change request, Kentucky’s Cabinet for Health and Family Services told KFF Health News.
Agency spokesperson Brice Mitchell said the change request was designed to address a “limitation of the system rather than technical issues.” The request, for which a second phase was implemented in July, cost $522,455 and took more than 3,500 hours of work, according to Mitchell and documents obtained in response to a public records request. All such requests “are thoroughly vetted, negotiated and approved by several areas within the Cabinet,” Mitchell said in an emailed statement.
“These are large, complex system implementations,” Walsh, of Deloitte, said. “So in all of them, you’re going to be able to find a point in time where there was an issue that needed to be fixed. And you can also find millions of people every day who are getting benefits through these systems.”
In February, Georgia officials were discussing a high-priority change request to resolve an ongoing problem: A defect affected potentially tens of thousands of “cases/claims” for families in the Supplemental Nutrition Assistance Program, known as SNAP, and the Temporary Assistance for Needy Families program that, among other problems, led the state to recoup some residents’ entire benefit, according to state documents KFF Health News obtained from a public records request. The programs provide monthly cash assistance to low-income people for food and housing. Georgia in 2014 inked a contract with Deloitte to build and maintain its eligibility system, known as Georgia Gateway.
Federal regulations cap how much money the government can recoup if a SNAP recipient was overpaid at 20% or $20, whichever is higher, according to legal aid attorneys and SNAP experts.
“We have plenty of clients who, that is their entire grocery budget,” said Adrianne Freeman, deputy director for litigation and advocacy at the Georgia Legal Services Program.
The defect — which Georgia DHS’ Brown said was identified on April 29, 2022 — created several problems, including incorrect calculations of how much to recoup and clawbacks not occurring on the correct start dates. “The Gateway system did not consistently adjust or apply the recoupment amount correctly,” Brown said.
A fix was deployed the weekend of Feb. 17, the documents state, but a formal change request was needed to “allow the State Agency (SA) to correctly apply allotment reductions to all SNAP and TANF cases impacted by Defect 21068,” the documents state. The change order would allow state officials to run an automated one-time mass update to fully resolve the problem.
The target date for doing so: March 1. That was nearly two years after officials were provided an “original report” noting that more than 25,000 cases may have been affected, the documents state.
Relying on Workarounds
States often face constraints on how many changes can be made in a year. In Texas, there is a years-long waitlist for changes, according to advocates, state documents, and the state health agency. “The system isn't nimble enough to meet the needs and often relies really heavily on manual workarounds,” said Stacey Pogue, a senior research fellow at Georgetown University’s Center on Health Insurance Reforms with expertise on Medicaid in Texas.
Texas eligibility workers use workarounds to process applications while awaiting permanent fixes. Deloitte said in its $295 million Texas contract that “there is a real need” for workarounds, which allow operations to continue “without affecting client benefits.”
Many of these “temporary” fixes were implemented years ago and were still in use in 2023, according to records obtained by KFF Health News that found 45 active workarounds in Texas last year. In one instance, a workaround was implemented nearly 14 years ago. Deloitte acknowledged in its Texas contract that reducing workarounds “is one of the top priorities.”
Smith of Deloitte said it doesn’t always take months to fix a problem: “We have changes that get implemented in a day and changes that get implemented in a month.”
Further, Smith said, Deloitte “is one part of implementing a change,” noting “we’re often not necessarily the constraint.”
The state considers several factors when assessing which fixes to tackle first, including how many beneficiaries are affected. The more complex the workaround, “the longer it may take for staff to process eligibility,” said Jennifer Ruffcorn, a spokesperson for Texas Health and Human Services.
In Florida — in addition to the lapses in coverage for maternal care — the National Health Law Program and the Florida Health Justice Project alleged in their lawsuit in federal court that notices to Medicaid beneficiaries alerting them their benefits would be terminated did not explain the basis for the decision.
In October, about a month after the lawsuit was filed, the state asked Deloitte to provide an estimate to alter the notices, Kallumkal of Deloitte testified at trial in August.
Deloitte estimated it would need roughly 28,000 hours, he said. That’s more than twice the 12,600 hours the state sets aside each year to pay Deloitte for revisions. The extra hours would require an amended contract in which the state would have to agree to pay more. Florida’s Department of Children and Families did not respond to requests for comment.
For Deloitte, extra hours mean more revenue, Kallumkal acknowledged during his testimony while under cross-examination. Deloitte subsequently provided the state with a new estimate for a narrower scope of work that would take 12,000 hours, he said.