Katheryn Houghton [CATH-er-in HOW-tun] reads the week’s news: New rules that require millions of Americans to work to access Medicaid are stricter than many expected. Plus, the federal Family and Medical Leave Act protects many people’s jobs — but there’s a big catch.
0:000:00
Speed
June 11
Sam Whitehead reads the week’s news: More Americans are getting access to physician-assisted suicide as states legalize the practice. Plus, hundreds of people allege medical neglect in ICE detention centers.
0:000:00
Speed
June 4
Arielle Zionts [arr-ee-ELL ZY-ence] reads the week’s news: For some older adults, the risks of certain preventive screenings might outweigh the rewards. Plus, cost spikes for Obamacare plans have consumers seeking cheaper health coverage, which is often less comprehensive.
0:000:00
Speed
May 28
Jackie Fortiér [FOR-tee-ay] reads this week’s news: Suicide prevention experts argue that improving Americans’ financial well-being could save lives. Plus, the Trump administration proposes looser artificial intelligence safeguards to speed innovation in healthcare.
0:000:00
Speed
The KFF Health News Minute is available every Thursday via direct download or the RSS feed.
Readers Curse Medical Debt and Defend Spelling Therapy
Your recent piece “Baffling. Frustrating. Frightening. What It’s Like To Be Sued Over Medical Debt” (June 1) adds to a growing breadth of firsthand patient experiences caused by undue medical debt. These patients understand they need to pay for their care but instead are strapped with baffling medical bills and no direct way to get assistance. That’s exactly what these hospital and insurer billing practices do: make it difficult for patients to understand what they are being charged for, leaving them to navigate uncertainty and frustration while trying to determine what they actually owe.
The National Consumers League has heard from patients and their caregivers who have daunting stories. Patients shouldn’t be at the mercy of unfair hospital practices or be forced to choose between vital medical treatments and other necessities because they’re priced out — but this is happening every day. NCL polling found that medical debt has affected most U.S. adults, with nearly half incurring this debt after receiving a “surprise” bill from a hospital or provider. These bills not only risk patients’ livelihoods and upend their financial stability, but they also ruin lives. When faced with medical debt, more than half of surveyed adults said they skipped future treatments or drained their savings.
There is also a correlation between hospitals that pursue medical debt and those participating in the federal 340B drug-pricing program. The intention behind 340B is to give hospitals and other eligible providers access to discounted medications so they can help reduce costs for low-income, uninsured, or otherwise vulnerable patients. Instead, 340B hospitals pursue aggressive medical debt collection practices at higher rates than their non-340B counterparts, explicitly failing to meet their end of the deal in 340B. Making matters worse, hospitals with high shares of cancer patients continue to use some of the most aggressive medical debt collection tactics.
Hospitals, especially those with heightened responsibilities to vulnerable patients, need to have transparency and accountability if they have the privilege of getting greatly reduced prices for drugs; the intention is to pass along those discounts to patients, not hoard the discounts. This is a federal program that needs a federal solution. Congress needs to step in and rein in these predatory medical debt collection practices. Until then, patients across the country will continue to suffer.
— Sally Greenberg, CEO of the National Consumers League; Washington, D.C.
We are defending a large number of medical debt cases here in Kansas. The unusual angle for us is the large number of cases brought to court with no attorney representing the debtor; most of those cases are default judgments. When we get involved, we learn most of the cases had improper service, so the party doesn’t know they’ve been sued.
One of our cases involves a mother of two who has been sued by a billion-dollar nonprofit hospital. Her paycheck at McDonald’s was garnished. We challenged their actions, and while the judgment has been set aside, the collection case is continuing.
— Matt Keenan, executive director of Kansas Legal Services; Topeka, Kansas
I don’t understand how the author of this piece was able to justify conflating camel’s milk and anti-vaxxers with people with whole-body apraxia being able to use the alphabet to spell out their thoughts and feelings. I find it incredibly disingenuous to lump together these unrelated topics to discredit or even bully severely disabled people and their families. And especially shameful is using hostile sources like Amy Lutz, who should know better than to try to demean parents who “subject” their children to the alphabet.
Offering a nonspeaker an alternative to silence and frustration that might otherwise lead to self-injurious and aggressive behavior is not dangerous. It’s not as if it’s some invasive, risky, or controversial treatment some parents are choosing to subject their loved ones to. It’s simply the alphabet and an alternative method of communication for individuals with whole-body apraxia. And it is real and not the imagination of pathetic families.
You are on the wrong side of history for all the wrong reasons, and, as the number of spellers and speller advocates grows, you will be ashamed and rightfully so.
— Joanne Curcio; Paramus, New Jersey
I am the father of Stone, a 20-year-old nonspeaking autistic young man who is currently carrying a 3.85 GPA in high school-level classes. Stone communicates using a keyboard, iPad, or letterboard, with support from a trained communication partner. He requires this support because of apraxia, a neurological condition that disrupts the motor pathway between thought and movement. His intelligence and his communication are not in question. His body’s ability to execute motor commands independently is the challenge, and that distinction matters enormously.
I am also the founder of Communicators for Communication Rights (C4CR) and host of The Lighter Side of the Spectrum podcast. I have spent years documenting the legal, scientific, and human case for communication access for nonspeaking individuals.
Your recent article does three things that cause real harm to the community I am part of and represent, and I want to name them directly.
First, it conflates motor-based communication with the Make America Healthy Again movement. This framing implies that letterboards and keyboard-based communication with a communication partner are a new initiative embraced primarily by parents who identify with the MAHA platform. Nothing could be further from the truth. These methods have been used and advocated for by families across the full ideological spectrum for decades. The article provides no data on how many of the families using these methods across the country are MAHA supporters. That is not a framing choice. It is a factual gap that mischaracterizes an entire population.
Second, the article focused on Elizabeth and Noah’s challenges with independent typing rather than examining what communication has actually brought to their lives. The assumption embedded in that framing, that authenticity requires independence, ignores the well-documented neurological reality of apraxia. These are not people choosing not to communicate independently. These are people whose motor systems do not reliably cooperate with their intentions. Holding them to a standard of independence that their neurology makes impossible, and then using that standard to question their communication, is the same mistake school districts make every day when they deny communication access to nonspeaking students.
Third, the article conflates motor-based communication with The Telepathy Tapes. That The Telepathy Tapes became a top podcast speaks to public interest in nonspeaking individuals and the stories told by Ky Dickens. It has nothing to do with whether nonspeaking people can communicate authentically through letterboards and keyboards. Bundling these two things together in the same piece suggests a connection that does not exist and gives ammunition to those who want to dismiss every nonspeaker’s communication as suspect.
When a credible news organization ties access to a political brand and a paranormal-focused podcast, it gives school districts a new weapon to use against nonspeaking students. The people who pay that price are not politicians. They are children sitting in classrooms without communication access right now.
— David Kaufer; Edmonds, Washington
Vexing Vaccine Research
Having read your article “A Danish Couple’s Maverick African Research Finds Its Moment in RFK Jr.’s Vaccine Policy” (May 18), my first question is: Why focus research on infants in Africa, Denmark, or minority populations in the United States rather than studying broader populations? What is the fascination with these groups and the rationale for selecting them?
I understand that vaccines may be administered at different ages in some countries due to limited availability and resources. If vaccine access is the issue, it seems that increasing immunization resources and availability would be a more direct solution.
I was born in 1961 and received the recommended childhood vaccinations of my time, on schedule. During my childhood, my family grew much of our own produce and purchased meat from local butchers and fishermen. Looking back, I do not recall autism being discussed or diagnosed as frequently as it is today. This leads me to wonder whether environmental and dietary changes deserve greater attention as potential contributing factors.
Over the decades, the food supply has changed significantly. Many processed foods now contain added sugars, corn syrup, artificial colorings, preservatives, and industrially produced oils. Modern agriculture and food production also involve pesticides, chemical treatments, and hormone use in some settings. At the same time, rates of obesity, diabetes, and autism diagnoses have increased. While correlation does not prove causation, these trends suggest that further research into environmental exposures, food production practices, and agricultural chemicals may be warranted.
For that reason, I question whether research efforts should focus primarily on vaccines as a possible explanation for autism or early childhood health outcomes. It may be equally important to investigate the food industry, farming practices, seafood production, crop treatments, and the long-term effects of environmental chemicals on children’s health.
I would encourage researchers — including Health and Human Services Secretary Robert F. Kennedy Jr., Denmark’s Christine Stabell Benn and Peter Aaby, and the Centers for Disease Control and Prevention — to pursue a broader examination of potential factors influencing autism rates and other childhood health concerns. Parents deserve research that explores all plausible causes and is conducted with transparency, scientific rigor, and respect for the communities involved.
I am also concerned about the ethical implications of conducting research in economically disadvantaged populations. Is this part of Project 2025 — or Jim Crow 2026? Any study involving infants and children should ensure informed consent, strong protections for participants, and a clear commitment to their well-being.
Ultimately, my concern comes from a desire to understand why autism diagnoses and other health challenges appear more common today than in previous generations. I hope researchers will continue to investigate all possible contributing factors and prioritize the health and welfare of children everywhere. It saddens me to think that our country is going backward.
What you described is something I saw repeatedly at the bedside. Patients often left the ICU with fragmented memories, vivid dreams, confusion, or little understanding of what had happened to them. The article rightly highlights the impact on patients. Equally important is the growing recognition that post-intensive care syndrome can affect families as well, known as PICS-F. They are often left carrying fear, unanswered questions, and the difficult task of trying to make sense of an overwhelming experience.
Your mention of ICU diaries as a potentially helpful tool is important. Research suggests they may help patients reconstruct their ICU experience, fill in memory gaps, and better understand what occurred during their hospitalization.
My observations led me to create a published ICU Diary for Families, designed not only to help patients piece together their ICU stay, but also to give families a place to track updates, write down questions, and organize information during a stressful and often confusing time. Later, I created a Hospital Wellness Journal for patients and families navigating hospitalization more broadly.
I created these resources because I repeatedly watched families struggling to remember physician updates and searching for some way to organize an experience that can feel deeply stressful and disorienting.
Although I no longer work at the bedside in critical care, my work continues to be shaped by what I saw there, through both my journals and artwork centered on healing and well-being.
Post-intensive care syndrome deserves broader awareness and continued attention to approaches that support not only survival, but recovery and understanding after critical illness.
— Nicole Cromwell; Carmel-by-the-Sea, California
Sandwiched Between Caring for Kids and Aging Parents? Reach Out for Resources
Being a family caregiver is hard work. On June 17, KFF Health News Midwest correspondent Cara Anthony joined WAMU’s Health Hub to discuss her experience with parenting while also caring for aging parents. Listen in as she shares tips for other members of the “sandwich generation.”
(DigitalVision/Getty Images)
Are you juggling the responsibilities of raising children and having aging parents?
Navigating that role can come with new responsibilities, stressors, and unexpected expenses, but claiming the caregiver identity can help. Researchers have found that people who identify as caregivers are more likely to use support services and feel a sense of community with others.
KFF Health News correspondent Cara Anthony joined WAMU’s Health Hub on June 17 to share her experiences as a parent with aging parents.
Listen to the Latest ‘KFF Health News Minute’
Listen to the Latest ‘KFF Health News Minute’
June 18, 2026
June 18
Katheryn Houghton [CATH-er-in HOW-tun] reads the week’s news: New rules that require millions of Americans to work to access Medicaid are stricter than many expected. Plus, the federal Family and Medical Leave Act protects many people’s jobs — but there’s a big catch.
0:000:00
Speed
June 11
Sam Whitehead reads the week’s news: More Americans are getting access to physician-assisted suicide as states legalize the practice. Plus, hundreds of people allege medical neglect in ICE detention centers.
0:000:00
Speed
June 4
Arielle Zionts [arr-ee-ELL ZY-ence] reads the week’s news: For some older adults, the risks of certain preventive screenings might outweigh the rewards. Plus, cost spikes for Obamacare plans have consumers seeking cheaper health coverage, which is often less comprehensive.
0:000:00
Speed
May 28
Jackie Fortiér [FOR-tee-ay] reads this week’s news: Suicide prevention experts argue that improving Americans’ financial well-being could save lives. Plus, the Trump administration proposes looser artificial intelligence safeguards to speed innovation in healthcare.
0:000:00
Speed
The KFF Health News Minute is available every Thursday via direct download or the RSS feed.
Arrests of Immigrant Parents Create Mental Health Crisis for Children
Damian Zermeño sits in the bedroom he used to share with his father. Damian is one of an estimated hundreds of thousands of children, most of them U.S. citizens, separated from a parent by the Trump administration’s immigration enforcement efforts. (Karla Gachet for KFF Health News)
Growing Up Scared
Arrests of Immigrant Parents Create Mental Health Crisis for Children
LOS ANGELES — Damian Zermeño, 15, sensed something was wrong the moment he got home from school.
His aunt sat at the dining table, sobbing. His father, who’d walked him to the bus stop that morning and promised to take him to dinner when he got back, wasn’t there.
Saúl Zermeño, a 45-year-old single dad, had gone to a routine check-in appointment at an Immigration and Customs Enforcement office that morning, a requirement he’d complied with for years. The father had deferred action that allowed him to stay and work in the U.S., according to his attorney. But that day, Oct. 3, officers deported him to Mexico, where he hadn’t lived since he was 9 years old. Zermeño had been Damian’s sole caregiver since he was a baby because his mother chose not to be involved in the boy’s life, the family said.
Suddenly, Damian, who was born in the U.S., found himself separated from his father by thousands of miles and a heavily guarded border. The previously cheerful 10th grader, who doesn’t have a driver’s license and can make a few basic dishes but isn’t used to cooking for himself, faced navigating his teenage years alone, his dad’s presence reduced to a two-dimensional image on his phone.
“I thought it wasn’t true,” Damian said. “I just went to my room. I didn’t want to leave. I didn’t even want to eat.”
Email Sign-Up
Subscribe to KFF Health News' free Morning Briefing.
Damian is among an estimated hundreds of thousands of children, most of them U.S. citizens, separated from a parent by the Trump administration’s deportation policies. Their mothers and fathers have been deported or locked for months inside detention centers, often miles away from where their families live. These children are separated, sometimes violently, from the adults they depend on. Parents have been arrested while dropping kids off at school, inside their homes, and at immigration check-ins with their children present. Most people detained have no criminal conviction. (Being in the U.S. without authorization is typically a civil offense). With their parents gone, kids’ lives are plunged into fear and uncertainty.
As a result, a generation of children from immigrant families are exhibiting mental health problems that could affect them for years.
Parents, therapists, and others who work with immigrant families said they’ve already encountered preschoolers with speech delays, elementary school children who talk of suicide, and teenagers too anxious to leave the house. Research has shown repeatedly that separating children from their parents harms their health and development. The stress of losing a primary caregiver creates havoc in a child’s brain and body, increasing their risk for mental and physical health problems, including depression, anxiety, post-traumatic stress disorder, a weakened immune system, and developmental delays.
“You can just see it in their faces; it’s almost like the light has been dimmed in their eyes,” said the Rev. Tanya Lopez, a pastor at Downey Memorial Christian Church who regularly visits immigrant families as part of a support organization made up of Los Angeles-area religious leaders.
The health risks from this stress response are long-term. People who experience parental separation and other traumatic events as children are more likely to have heart disease, diabetes, cancer, and other chronic conditions as adults.
In a statement, the Department of Homeland Security said ICE does not separate families, and that parents are asked if they want to be removed from the country with their children or to designate a safe person for them to stay with in the U.S.
However, a report by the Women’s Refugee Commission and Physicians for Human Rights found that many parents aren’t given that choice, and that ICE often doesn’t ask detainees if they have children or take steps to ensure that children left behind are safe. Saúl Zermeño said ICE officers didn’t ask about his son or check on Damian’s well-being when he was deported.
Damian Zermeño at a birthday celebration a few months before his dad, Saúl Zermeño (right), was deported to Mexico. Damian is one of an estimated hundreds of thousands of children separated from a parent by the Trump administration’s deportation policies. Many of these children suffer mental and emotional health problems as a result. (Claudia Zermeño)
For days after his father’s deportation, Damian didn’t want to leave his room, eat, or go to school. He stopped talking to his friends. He stopped playing his favorite video game, Fears To Fathom. When he returned to school a week later, the teenager would cry in class or walk out overwhelmed with sadness. Even his favorite subject — English — lost its appeal.
Damian and his father were inseparable; family members joked that they never saw one without the other. Zermeño took Damian, who has attention-deficit/hyperactivity disorder, autism, and other health conditions, to his medical appointments. He cooked for him and combed his hair. He loved to take Damian to his favorite Thai restaurant or to get boba drinks after school. As much as they joked around and played pranks on each other, Zermeño also taught Damian the importance of work by bringing him along to construction jobs and to find supplies at Home Depot.
Damian used to get annoyed with his father’s motivational chats about responsibility. Now they’re one of the things he misses most.
“I thank my dad every day for teaching me to be strong before he left,” Damian said.
Damian talks to his father over video chat. Saúl, a single parent, was deported to Mexico in October after living 36 years in the United States. Now, the only way the two see each other is through a screen. (Karla Gachet for KFF Health News)
Elsewhere in Los Angeles, Jacob, a shy 9-year-old with cropped, curly hair, skinny limbs, and a serious expression, was missing his mom. On a Saturday in May, he clung tightly to his father’s hand as they walked among homeless people, street peddlers, and the stench of urine that hangs in the air outside the building where they live in a cramped apartment. He hoped his mom would soon be released from immigration detention so that he could hug her again.
“If my mom was here, I’d be happy,” he said. “Right now, I’m not.”
Jacob is in some ways a typical 9-year-old. He likes playing Roblox and Street Fighter. He dreams of becoming a police officer and of owning a guard dog, “because you can train them and they defend you.”
But he also endured a harrowing journey, even before being separated from his mom in January. Jacob’s family fled their home country of Colombia in 2024 because members of a paramilitary group threatened to kill them, his father, Andreis, said. During their journey to the United States, Jacob saw dead bodies while trekking through the jungle, was kidnapped and robbed at gunpoint with his parents, witnessed a rape, and had to sell candy and beg for money, his dad said. KFF Health News is not using the father’s or son’s real name because the family fears it would jeopardize their asylum cases.
After the family arrived in Los Angeles, Jacob suffered from nightmares and an intense fear of being alone. He started to recover once he began attending school and got connected to therapy through the school district, his dad said. For a short while, the family felt they had found peace.
Then, immigration officers detained Jacob’s mother at a check-in appointment while he and Andreis sat in the waiting room. The mother has a pending asylum application and no criminal record, Andreis said. The father said he and his son broke down when officers informed them of his wife’s detention, handing them a bag with her wallet and cellphone. They returned home without her, leaving Jacob inconsolable.
“He was terrified,” the father said, fighting back tears, his voice growing quiet as he recounted that moment. “He was crying with rage.”
After that, Jacob didn’t want to eat or go to school. When he went to school at his dad’s insistence, his teacher called home to ask why he was crying in class. Jacob couldn’t sleep. He acted out. He blamed his dad.
“When will my mom come back?” he asked his dad. “Why do they have my mom? I miss my mom.”
At the same time, Andreis said, he was going through his own crisis, trying in vain to console his son while wrestling with grief, worry, and desperation over what happened to his wife. He stopped his work as a laborer for two weeks to take care of Jacob, but that created financial stress and meant he sometimes couldn’t afford to fund his wife’s commissary account so she could buy better food and make phone calls. Jacob lived for those phone calls.
Jacob listed all the things he missed about his mom, including her cooking (rice with meat, corn cakes with egg), visiting the park together, and her taking him to get his hair cut, treating him to McDonald’s on the weekend, and bringing him to church. Most of all, he missed being close to her.
“I would lie down with her, and I’d watch videos with her,” he said. “My mom would hug me and I’d hug her.”
Sometimes he sprayed her perfume on himself so he could smell her.
After almost five months at the Adelanto ICE Processing Center, Jacob’s mother was released based on a habeas corpus petition in May. The family is still living in fear of detention or deportation. The father worries he too could be detained, and what that would mean for Jacob. Andreis is currently appealing a removal order for the two of them.
A recent analysis published by the Brookings Institution estimates that over 200,000 children — including 145,000 U.S. citizen children — have likely had at least one parent detained since President Donald Trump returned to office. About a third of those children are under age 6. The number of children with detained parents is expected to grow as the federal government pours over $200 billion into immigration enforcement, including funding from the GOP’s One Big Beautiful Bill Act and a $70 billion appropriation Trump signed this month.
More than 4.6 million U.S. citizen children live with a parent at risk of deportation, according to the report.
Families Broken
Noemi, a Guatemalan mother and asylum seeker, stood in the parking lot at an ICE office north of Los Angeles, her three children wailing and clinging to her, glass from the family’s car scattered at their feet.
Moments earlier, immigration agents had smashed a window and forced her partner out of the car while he waited for Noemi and the kids to finish a check-in appointment. While they were inside, officers tried to separate Noemi from the couple’s children, ages 9, 7, and 1, but gave up after the kids started screaming, Noemi said. Meanwhile, her partner, a Mexican national who’s lived in the U.S. for almost 20 years, was sent to the ICE detention center in Adelanto.
“It was something tragic, something inexplicable that happened that day,” said Noemi, who asked to withhold her full name because she fears government retaliation for sharing her story. “It’s something that marks you for your whole life. My family was broken.”
Located in the Mojave Desert, the privately run Adelanto ICE Processing Center is the immigration detention center closest to Los Angeles and one of the largest in the U.S. It held a daily average of over 1,700 people as of April, and a facility next door called the Desert View Annex held an additional 426.
Since her partner’s detention in December, Noemi said, their children haven’t been the same.
Her 7-year-old daughter, till then usually happy and smiling, became depressed and refused to eat. Her once-high grades plummeted, and she forgot the names of letters and numbers in both English and Spanish. She and her 9-year-old brother struggled to sleep and asked constantly about their dad, wondering if he was taken because they’d done something wrong.
“Why is this happening to us?” they asked her. “We’re good. We’re studying.”
Noemi’s youngest daughter went back to crawling for three months, even though she’d already learned to walk before her father was taken. The little girl would cry out in her sleep, “Pa! Pa!”
Sofia Mendoza, a therapist who works with immigrant families at a community clinic in Los Angeles County, said separated children can experience a form of grief. It’s hard for them to come to terms with their parent’s absence because the parent is still alive, but not with them. This can disrupt the child’s bond with that parent and their ability to form trusting relationships in the future, she said.
Many children also become extremely anxious, angry, and fearful, Mendoza said. Young children often complain of physical symptoms such as stomachaches, develop separation anxiety, and regress to earlier behaviors like bed-wetting. Older children may have panic attacks, nightmares, and difficulty focusing, Mendoza said. Caregiver loss is also associated with increased risk of suicide and substance use in children.
Norma Gómez, a project manager for the Mixteco Indigena Community Organizing Project in Oxnard, said after immigration raids shook the community last summer, her 9-year-old daughter refused to go to school for a week and was afraid to leave her mom and dad, even though they’re legal U.S. residents. She’d seen other kids at school crying because family members had been detained. Gómez showed her daughter their U.S. residency documents to reassure her. The child asked to make copies for her classmates, hoping they would protect them too.
‘Time To Be an Adult’
Back in East Los Angeles, Damian is living with one of his aunts and struggling to adapt to not having his father around. He said his grades have dropped because he can’t focus in school. He no longer wants to do things he used to enjoy with his dad, such as going out to eat.
“Fun is over,” he said. “It’s time to be an adult right now.”
Damian embraces his aunt Claudia Zermeño, who has taken legal guardianship of him since his father was deported to Mexico. She’s caring for him, her two children, and her mother. (Karla Gachet for KFF Health News)
Damian’s aunts prepare lunch at the home the 15-year-old shared with his dad. (Karla Gachet for KFF Health News)
The two women have stepped in to take care of Damian, who has numerous health issues, since their brother was deported. (Karla Gachet for KFF Health News)
Being without his father has forced Damian to become more independent, he and his aunt Claudia Zermeño said. Before, his dad did almost everything for him. Now, Damian does his own laundry, helps with housework, and styles his own hair. He’s protective of his aunts, who are both devastated by their brother’s absence; he hugs them frequently and tells jokes to try to cheer them up. He doesn’t want to upset them more by showing his own sadness.
Damian receives therapy both in and outside of school. He said he’s learned breathing exercises that have helped, but he still feels sad and worried a lot of the time. Sometimes he feels angry.
“I try my hardest to think, to stay focused,” he said. “But with everything that’s going on, I can’t keep the facade of ‘everything’s normal’ when I feel heartbroken.”
Saúl Zermeño, now living in Guadalajara, said he’s worried about his son’s health. Damian has a genetic condition called neurofibromatosis Type 1, which causes tumors to grow on nerve tissue in his body, including one in his head that, if not checked regularly by a doctor and monitored by his family, could interfere with his brain. He also suffers from epilepsy and was born with only one kidney, which means he tires easily and doesn’t play sports. Saúl is afraid his son won’t get the care he needs without him there. As Damian’s legal guardian, Claudia Zermeño is doing everything she can for him, but she has two children of her own and is also caring for her mother, who has neurological problems from a stroke.
Damian talks with his dad as often as he can. He hopes to visit his father in Mexico, but he doesn’t have a passport and, as a minor under 16, there are more requirements to get one without his dad present. Saúl is working with an attorney to get permission to legally return to the U.S., but the process is complicated and uncertain.
So, for now, Damian’s hanging on to hope that his dad will be allowed to return and is trying to become the man he believes he should be. He’s making plans to get his driver’s license when he turns 16 this month. He’s given up his goal of going to college and instead wants to get a job right after high school to help his aunts and send money to his dad.
He still cries, but only when he’s alone in his room.
Damian talks to his father over video chat. (Karla Gachet for KFF Health News)
More Americans Are Surviving Cancer. But the Mental Health Challenges Can Persist.
More Americans Are Surviving Cancer. But the Mental Health Challenges Can Persist.
Morgan Newman was diagnosed with stage 3 cervical cancer at age 24 but has been free of cancer for a decade. She says she still deals with lingering fears of the cancer returning. (Natalie Krebs/Iowa Public Radio)
The cancer diagnosis came as a shock, disrupting Morgan Newman’s plans for launching her life. It was 2015, and she was working as a dental assistant in Des Moines, Iowa, while studying to become a social worker.
After an abnormal result on her Pap smear, her doctor brought her back in to check the tissue for signs of cancer. Newman wasn’t that concerned at first. She was only 24 years old.
“I didn’t think anything of it,” she said. Friends had received abnormal results, she recalled, “and they turned out to be OK.”
But during the follow-up examination, she started bleeding so heavily that the doctor stopped the exam and immediately referred her to a gynecologic oncologist. Newman soon learned she had cervical cancer. She had just moved into her own apartment for the first time.
An increasing number of Americans are getting — and surviving — cancer. There were more than 18 million cancer survivors in the U.S. in 2025, and the National Cancer Institute estimates that number will grow to 22 million by 2035. But long after completing treatment, many survivors face lingering mental health challenges that go unaddressed.
Newman underwent six weeks of radiation and chemotherapy. Her scans after that were clear until the six-month mark, when her doctors found suspicious nodules in her lungs.
Newman endured additional chemotherapy, which had more side effects. It was physically exhausting. But she was also struggling psychologically as she watched her friends hit significant adult milestones.
“My friends were getting married, they were having children, you know, progressing in their lives and their careers, and I just felt stuck,” she said.
Newman had done therapy before, for anxiety and depression. But after she got sick, she had to quit. Therapy was too expensive now that she had her other medical bills. And amid the doctor appointments, college courses, and her full-time job, she didn’t have the time.
Newman’s cancer treatment ended, and the scans remained clear. By 2017, she had a new job with better health benefits. So she decided she could go back to therapy.
She worried that every ache and pain could be the cancer coming back. At times, it was emotionally difficult to spend time with her friends who had kids, because the radiation treatment had damaged her reproductive system, leaving her unable to have her own children.
Now, almost 10 years later, Newman remains free of cancer, and cancer prevention has become her passion. She started a new job in December as the Iowa grassroots manager for the lobbying arm of the American Cancer Society, and she has served on the boards of other cancer organizations in Iowa.
But she continues to go to therapy to deal with the lingering anxiety, as well as the lingering effects of her treatment, such as her infertility.
“The fear of the unknown really takes over and can physically impact your body, as well as your mind,” she said. That question kept circling: “What if the cancer is back?”
Email Sign-Up
Subscribe to KFF Health News' free Morning Briefing.
Cancer’s ‘Silent’ Impacts
Studiesshow cancer survivors experience anxiety and depression that can last years after they finish treatment.
The advocacy group Cancer Nation surveyed patients nationwide last year. It found that about a third of those who had finished treatment reported anxiety about their cancer potentially coming back, as well as problems with not feeling like their “old self.” Only 1 in 5 of the surveyed survivors reported seeing a mental health professional.
Finding therapists who understand how cancer can affect people physically and emotionally can be a challenge, especially in states like Iowa. According to the Iowa Cancer Registry, the number of Iowans living five years after their diagnosis has increased about 0.4% each year since 2000, and the state has the second-highest rate of new cancer diagnoses. Researchers aren’t sure why, but the University of Iowa scientists who run the registry are taking a deep dive into the issue in a two-year, state-funded project.
Iowa is also largely rural. Some of the counties that have the highest cancer rates also have the fewest mental health workers. Newman went through several therapists before she was able to get an appointment with Julie Larson, a Des Moines-based therapist who works with a lot of cancer survivors.
“I just felt like I needed something more specific to what I was going through,” Newman said.
In Larson’s practice, it’s common for clients like Newman to start therapy months or even a year after finishing treatment, when they realize they aren’t feeling how they expected to feel.
“Physically, people’s bodies have changed,” Larson said. “And they are reconciling loss and grief. And those experiences are a little bit more silent, a little more invisible, and friends and family don’t often fully understand or grasp that.”
Larson said cancer survivors often seek her out because she understands cancer and the different forms of treatment people may have experienced.
“I’m not a doctor, but I’ve done this a long time. So I know what happens when people have Adriamycin. I know the treatment protocol for carboplatin,” she said, citing chemotherapy drugs.
Richard Deming, medical director at the MercyOne Richard Deming Cancer Center in Des Moines, Iowa, says the clinic has recently added services such as yoga and counseling to help cancer patients and survivors deal with mental health issues. (Natalie Krebs/Iowa Public Radio)
Oncology and Mental Health
When it comes to treating cancer, the field of oncology often neglects mental health, said Patricia Ganz, an oncologist and professor at the UCLA School of Public Health who has spent decades doing research on cancer survivors and their lingering challenges.
“We know how to give pills. We know how to give pain medicine, sleep medicines. But we’re not really schooled in the antidepressants,” she said.
There’s an increasing awareness about the need to screen for psychological distress in cancer patients and the need to provide mental health services for cancer patients and survivors, Ganz said, but expert-recommended screenings and referrals don’t always happen to the extent they should.
“You get cared for intensely when you’re getting treated for cancer,” said Richard Deming, the medical director at the clinic named for him. By contrast, he said, when people complete treatment, the care typically shifts: “It’s almost like, ‘You should feel fortunate that you’re cancer-free and just get on with your life.’”
To treat cancer comprehensively, Deming said, doctors need to pay attention to far more than just physical symptoms. That requires a shift in the way doctors treat patients, he said.
“Every step along the way, whether it’s through diagnosis or treatment or follow-up, we have to ask, ‘What are the issues you’re experiencing?’” Deming said. “Not just: ‘Do you have cancer? Did we get rid of the cancer?’”
This article is from a partnership that includes Iowa Public Radio, NPR, and KFF Health News.
Democrats Seek To Spotlight Rising Health Costs by Forcing Vote on Trump Regulation
Democrats Seek To Spotlight Rising Health Costs by Forcing Vote on Trump Regulation
Sen. Tammy Baldwin and other Democrats in the Senate are seeking to overturn a Trump administration rule they say will hamper Obamacare coverage. (Kayla Bartkowski/Getty Images)
In a move that mixes pure politics with weedy congressional procedures, Senate Democrats are seeking to force a vote to overturn a Trump administration rule that they say will make it harder to enroll in Affordable Care Act health plans and sharply raise out-of-pocket costs for those who do stay covered.
The measure is unlikely to pass in the Republican-controlled Congress, but Democrats could use the vote against their opponents on the campaign trail.
When the ACA rule was released in May, the Trump administration touted it as a means to combat enrollment fraud, lower premiums for some people, and offer a wider range of insurance plans, including ones with no set network of doctors or hospitals.
But many Democrats warned the changes would hurt consumers already suffering from high healthcare costs as well as higher prices for gas, groceries, and other household needs. Estimates from the administration found the regulation, called a notice of benefit and payment parameters, could cause up to 2 million people to lose ACA coverage.
Senate Minority Leader Chuck Schumer and fellow Democratic Sens. Tammy Baldwin of Wisconsin and Ron Wyden of Oregon plan to introduce on Wednesday a Congressional Review Act resolution to block the rule.
Baldwin told KFF Health News in a statement that the rule is “misguided” and said she was “committed to doing everything she can” to stop Republicans from “kicking Americans off their health care.”
Email Sign-Up
Subscribe to KFF Health News' free weekly newsletter, "The Week in Brief."
The directive from the Centers for Medicare & Medicaid Services is an annual exercise that sets standards for ACA coverage during the coming year. Some of the changes in the finalized 2027 rule are technical, but many would affect consumers directly.
They include tighter income verification requirements. The rule also stipulates more eligibility checks on people applying outside of the normal annual enrollment period for such reasons as marriage, divorce, or loss of job-based coverage.
ACA plans themselves would look different too. Insurers would be able to offer some plans with 30% higher out-of-pocket limits (the amount consumers may have to pay each year in cost sharing such as copayments and deductibles), with a new ceiling as high as $15,600 for individual coverage or $31,200 for a family plan.
The Democrats’ effort to overturn the rule is the definition of a long shot; it would need a majority of votes in both the House and the Senate. But simply forcing a floor vote is likely to be seen as a win by the minority party.
“What Democrats are trying to do is get Republicans to vote on policies that would be unpopular if they rose to the level of public consciousness,” said Adrianna McIntyre, an assistant professor in the Department of Health Policy and Management at the Harvard T.H. Chan School of Public Health. “Democrats want to showcase that they want to change these policies, even if don’t have the votes to accomplish it.”
Congress has authority under the review act — enacted as part of a larger law in 1996 — to overturn rules issued by federal agencies. While more than 40 such disapproval resolutions have passed, hundreds have been introduced, often mainly to draw attention to an issue.
It is one of the few levers a minority party has to force action on the floor of the Senate.
That’s because if only 30 senators sign a discharge petition to send the measure to the floor, the Democrats get a vote, without needing to go through a Republican-controlled committee or hold a hearing. A companion resolution is expected to be introduced in the House on June 17.
And there’s no doubt that Democrats will try to use any floor vote on health costs as a litmus test for Republicans in the November elections.
“Time and again Democrats have used Republican efforts to undermine the ACA to their political advantage in campaigns, and this year will be no different,” said Larry Levitt, executive vice president for health policy at KFF, a health information nonprofit that includes KFF Health News.
Polls show that the GOP could be vulnerable if Democrats can convince voters their party would do better on health costs, which are a top concern among voters.
A recent Pew poll, for example, found that 73% of adults see healthcare costs as a very big problem for the country, leading both inflation and the federal budget deficit. KFF’s tracking polls have found healthcare costs to be a top concern, even among Make America Healthy Again supporters allied with President Donald Trump.
At least half of people who identify as MAHA voters say those health costs will have a “major impact” on their decision to vote and which party they support.
Medical costs in general typically rise faster than inflation, driven by increased hospital and doctor bills and use of drugs, devices, and other healthcare. That leads to higher costs for employers that offer health plans to their workers and for taxpayer-supported programs such as Medicare and Medicaid, as well as higher premiums for insurance plans sold under the ACA. The consultancy PwC projects the cost to treat patients this year will rise by 9%, the highest in nearly two decades.
Higher premiums and lower subsidies also hit many ACA enrollees this year, with about 1.2 million fewer sign-ups than for 2025 as of January.
Costs “are a good Democratic talking point,” said Joseph Antos, a former government health official who is now a senior fellow emeritus at the right-leaning American Enterprise Institute. “Trump was going to solve inflation, and instead, what do we have?”
Tennessee Pharmacies Sell Potent Ivermectin, Led by Anti-Vaccine Doctor Who’s Taken ‘Bucketloads’
Tennessee Pharmacies Sell Potent Ivermectin, Led by Anti-Vaccine Doctor Who’s Taken ‘Bucketloads’
The physician has fueled sales of the controversial drug in the Volunteer State, where it can now be dispensed without requiring a doctor visit.
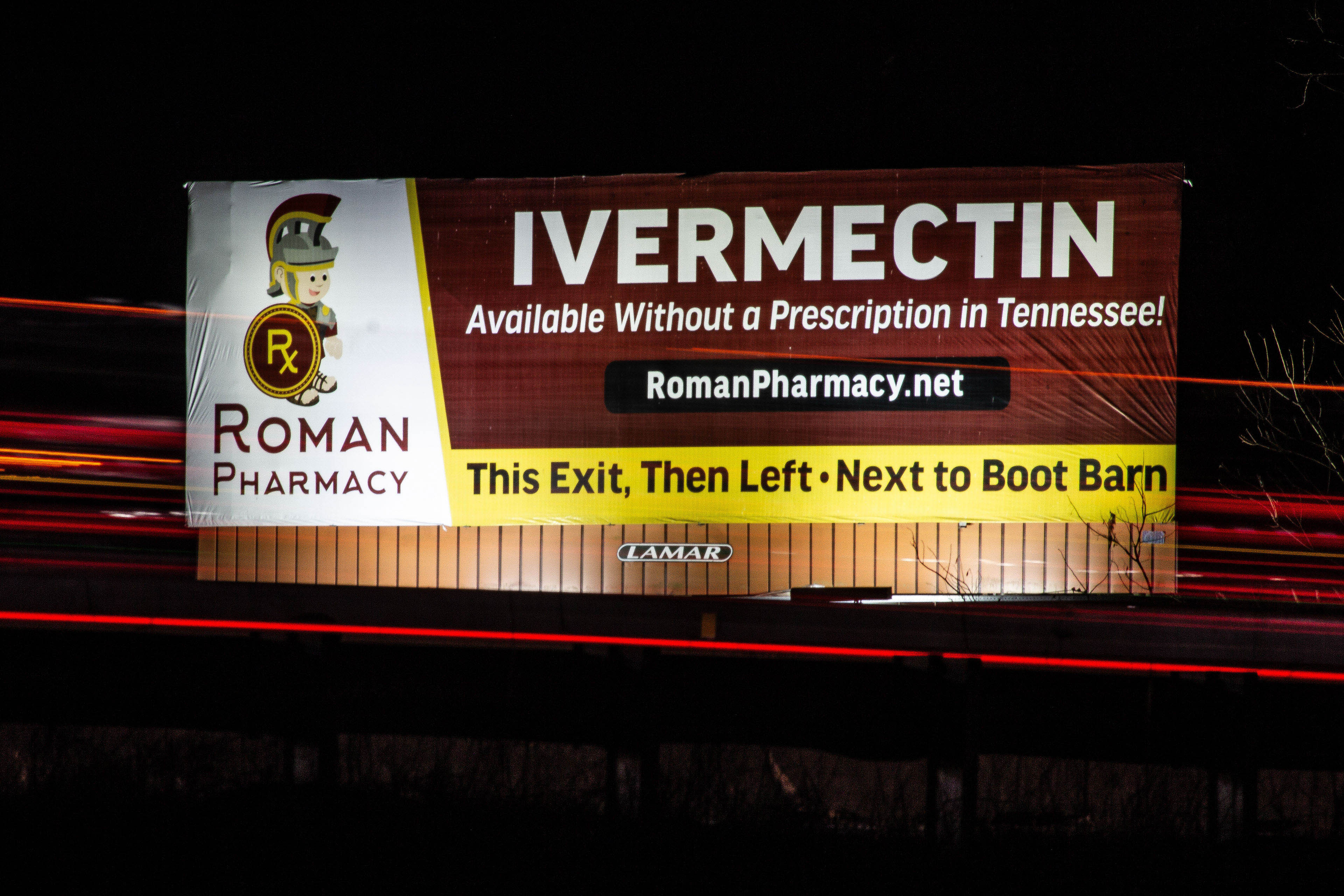
Roman Pharmacy advertises ivermectin on at least four billboards along Interstate 65 near Nashville. In 2022, Tennessee became the first state to allow ivermectin to be sold without patient-specific prescriptions. (Brett Kelman/KFF Health News)
Tennessee Pharmacies Sell Potent Ivermectin, Led by Anti-Vaccine Doctor Who’s Taken ‘Bucketloads’
The physician has fueled sales of the controversial drug in the Volunteer State, where it can now be dispensed without requiring a doctor visit.
NASHVILLE, Tenn. — Four years ago, Tennessee became the first state to allow adults to buy the antiparasitic drug ivermectin from a pharmacy without first seeing a doctor. Pharmacies can use a pre-written, blanket prescription to sell to just about anyone who walks through their doors.
The drug is now marketed and sold across the state in roadside shops and small-town strip malls with little oversight from health authorities. Highway billboards advertise ivermectin as “Available Without a Prescription in Tennessee!” while dozens of pharmacies offer highly concentrated pills, sometimes at 10 or 20 times the potency of a standard tablet.
Ivermectin is a Nobel Prize-winning, generally safe drug approved by the FDA for treating parasitic diseases in humans, which can generally be done with a single dose of three or four prescription-strength tablets. It is also used as a dewormer for horses and other livestock.
Its popularity surged during the pandemic as fringe doctors and anti-vaccine activists promoted it as a treatment for covid. Clinical trials have shown that ivermectin is not effective against covid.
Nonetheless, it has since become a symbol of resistance against the medical establishment among conservatives and followers of the Make America Healthy Again movement, championed by Health and Human Services Secretary Robert F. Kennedy Jr.
Timothy Caulfield, a professor at the University of Alberta who studies health misinformation, said ivermectin became an “ideological flag” during the covid pandemic, opening the door for influencers to push the drug for other ailments to a “captured audience” even without proof it works for those conditions.
“This is really about profit. This is about political identity. This is about creating distrust in the existing biomedical community. This is about money,” Caulfield said in an interview with ABC News, which partnered with KFF Health News to report on ivermectin.
After a hantavirus outbreak on a cruise ship earlier this year, unproven claims that ivermectin is effective against the virus have been spread by some popular social media accounts and right-wing figures, including former congresswoman Marjorie Taylor Greene. The World Health Organization says it has seen no research that shows ivermectin is an effective hantavirus treatment.
Tennessee’s ivermectin bill was shepherded by a Republican supermajority in 2022. Its passage blindsided state medical officials and handed a victory to medical groups that spread covid misinformation.
Some pharmacy websites now offer the drug as a treatment for covid, “long haul vax symptoms,” diabetes, or cancer — despite no evidence of its effectiveness for those purposes — while the new law largely gives pharmacists immunity from lawsuits or professional sanctions related to ivermectin.
The law was also a harbinger of legislation to come: More than two dozen states have since considered look-alike bills that would make the politicized medication available without a requiring a doctor visit.
John Mafi, a UCLA internal medicine physician who has studied the rise of ivermectin among cancer patients, worries it will lure people away from proven treatments. He co-authored a new study identifying a sharp increase in prescribing rates for ivermectin and another antiparasitic drug, particularly in the South. The rise followed a January 2025 episode of the Joe Rogan Experience podcast in which actor Mel Gibson claimed ivermectin and other drugs cured three friends with stage 4 cancer.
“It’s going back to 19th-century quack science,” Mafi said about off-label use of ivermectin. “It is alarming that I’m seeing this really unproven therapy being touted to so many potentially vulnerable Americans.”
Concentrated ivermectin pills like these are sold at compounding pharmacies across Tennessee. Under a 2022 law that made the drug available to people without requiring a doctor visit, some pharmacies offer pills that are 10 or 20 times the strength of standard ivermectin tablets. (Brett Kelman/KFF Health News)
The FDA says ivermectin can be dangerous in large doses. Tennessee has seen a small but concerning rise in signs of overuse. The Tennessee Poison Center, which fields calls from people exposed to drugs or toxic substances, received more than 60 calls for possible ivermectin poisoning in 2025, the most since 2021. They included reports of vomiting, blurred vision, neurological problems, and difficulty walking.
“People are taking this because they just feel unwell. It’s almost like a panacea now,” said Rebecca Bruccoleri, the poison center’s medical director. “I’ve heard rumblings on the internet of using ivermectin for an alternative cancer treatment, and we’re seeing it definitely in here.”
Pharmacist Paul Hughey has dispensed ivermectin under the new law at two Tennessee pharmacies: Mt. Juliet Pharmacy and Compound Rx. He estimated that “up to 20 people in a week” are buying ivermectin but that peak demand was double or triple that amount.
For years, Hughey said in an interview, customers have relayed emotional “testimonies” about the drug healing the sick, “especially with the cancer patients.”
“I’ll get a doctor call in and they say: ‘Guess what. So-and-so is cured.’ And it’s just amazing to hear that. So anybody who doubts that,” Hughey said, “I don’t really know that they’re practicing medicine. I think they’re just following the narrative.”
Email Sign-Up
Subscribe to KFF Health News' free Morning Briefing.
‘I’ve Taken Bucketloads of This Stuff’
The linchpin of Tennessee’s ivermectin market is Denise Sibley, a conservative doctor who was instrumental to the creation of the 2022 ivermectin law. She has inked agreements with pharmacies across the state empowering them to sell the drug.
Tennessee’s law allows pharmacies to dispense ivermectin without a specific prescription for each patient, through a “collaborative pharmacy practice agreement” with a doctor who provides what is functionally a pre-written, nonspecific prescription for all potential customers.
In podcast interviews, Sibley has said she has made as many as 40 of these agreements with Tennessee pharmacies, which she said forward her the paperwork on each ivermectin customer. Before selling the drug, pharmacies are required to ask customers questions about medical conditions and medications that could cause complications if taken with ivermectin. Afterward, the collaborating physician also is expected to receive a record for each person who purchases ivermectin.
“We literally have folks coming from all over the world to get our ivermectin,” Sibley said on the Common Sense MD podcast in February 2025. “As the collaborator for these pharmacies, I get every person’s sheet.”
“They’re from every state,” she said. “They’re from Canada. They’re from Europe.”
Sibley did not respond to requests for comment.
Denise Sibley, a doctor and vaccine opponent, testifies before Tennessee lawmakers in favor of the state’s 2022 bill allowing ivermectin to be offered without a specific prescription for each patient. Sibley has since signed agreements that empower numerous pharmacies to dispense ivermectin this way. (Tennessee General Assembly; screenshot by KFF Health News)
KFF Health News has independently confirmed that Sibley signed agreements with at least 10 pharmacies. The agreements say pharmacists shall dispense ivermectin only in Tennessee, where Sibley is licensed, although one of those pharmacies said friends and family in Tennessee can “facilitate sending the medication.”
Hughey, the Tennessee pharmacist, said Sibley had prescribing agreements ready to go when the law was enacted. He credited her with advancing ivermectin sales throughout the state.
“Had Dr. Sibley not stepped in and really pushed forward, there’s no telling how hard it would have been,” Hughey said. “It would have been a lot less widespread.”
Sibley also works with Children’s Health Defense, the Kennedy-founded group that has become one of the nation’s most influential anti-vaccine organizations. In podcasts, Sibley has referred to the covid vaccine as a “bioweapon” and “the most toxic substance that’s ever been produced.”
Separately, she testified before Tennessee legislators in 2024 about an alleged plot to change the weather and block sunlight. The New York Times then included her in a story about conspiracy theorists.
Sibley has said in podcast interviews that she was told by God to treat covid patients. She said she has advocated for ivermectin ever since.
“God agrees with what I’m doing,” Sibley said in 2023 on the podcast Tomi Lahren Is Fearless, which is recorded in Nashville. “I wake up every day and I say: ‘Yes, sir. I’m reporting to duty.’”
In legislative and government hearings throughout 2022, Sibley testified that she had treated around 4,400 people with ivermectin, including some Tennessee lawmakers, all without taking payment. Sibley described ivermectin as “a wonder drug” and said making it more available “would help me to save lives.”
“I’ve taken bucketloads of this stuff myself,” Sibley said in one such hearing. “I feel like I’ve been a good test subject.”
Sibley has said she dispenses ivermectin using treatment guidelines developed by Paul Marik, who in 2020 co-founded the Independent Medical Alliance, a medical group that has promoted ivermectin as an effective treatment for covid, flu, RSV, and cancer.
Some Tennessee pharmacies now follow those protocols, too. The protocols recommend patients take 1.5 to five times as much ivermectin as is normally prescribed to treat parasites, with the dose taken for days or weeks instead of just once.
Marik and other ivermectin proponents sued the FDA in 2022 after it discouraged the use of the drug for covid by tweeting: “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” The agency settled the lawsuit with no admission of wrongdoing and deleted the viral tweet in 2024.
The American Board of Internal Medicine has revoked Sibley’s and Marik’s board certifications but declined to explain why. Sibley still holds a Tennessee medical license; Marik is based in Virginia and is not licensed. Sibley and Marik eachopposed the internal medicine board’s actions.
In response to questions from KFF Health News, Marik, through an Independent Medical Alliance spokesperson, said medical science benefits from “open discussion of ideas and treatments.”
“Many independent doctors have reported that treatments like Ivermectin, in conjunction with traditional treatments, are showing promise. These ideas should be explored,” alliance spokesperson Lynne Kristensen said in an emailed statement.
Marik testified in favor of Tennessee’s ivermectin legislation in 2022, telling lawmakers that it is necessary because people would otherwise buy animal-grade ivermectin in stronger dosages meant for livestock.
“They’re buying ivermectin from farm stores. We don’t know the quality,” Marik said at a March 2022 legislative hearing on the Tennessee bill. “So this would prevent that from happening.”
One study identified a sharp increase in prescribing rates for ivermectin after a January 2025 episode of the Joe Rogan Experience podcast in which actor Mel Gibson claimed ivermectin and other drugs cured three friends with stage 4 cancer. (Brett Kelman/KFF Health News)
Tennessee Does Not Track Its Ivermectin Market
Arkansas, Idaho, Louisiana, and Texas enacted similar laws in 2025, and legislation that makes ivermectin available without the need for a doctor visit has been introduced or debated in at least 24 other states, according to a KFF Health News analysis. That means half the country could be following Tennessee down an unlit path, because no one knows the full scope of its ivermectin market.
Tennessee does not effectively track which pharmacies offer ivermectin this way, and the state government has been unable to produce some foundational documents that pharmacies are legally required to file before they sell the drug, according to a KFF Health News investigation.
Doctors and pharmacies are required by law to notify the Tennessee Department of Health when they sign agreements that allow ivermectin to be dispensed without patient-specific prescriptions, although it is not clear whether this consistently occurs.
In response to a KFF Health News public records request for those ivermectin notifications filed by pharmacies, the agency over three months produced records from only 12 pharmacies, half of which have agreements with Sibley. The agency said it did not locate records related to at least 13 others that KFF Health News has identified as selling ivermectin without requiring individual prescriptions.
Department of Health spokesperson Dean Flener said the agency would not answer questions about whether or how it regulates ivermectin or the pharmacies that distribute it.
Tennessee has said it does not track how much of the drug is sold in the state, and the amount is not well captured by federal or insurance data sources. That’s because the drug is often sold at compounding pharmacies, which make customized medications that are not FDA-approved and rarely covered by insurance. Drugmakers and wholesalers did not respond to questions about how much ivermectin they supply to pharmacies in the state.
Even the Independent Medical Alliance, one of ivermectin’s biggest cheerleaders, says it doesn’t know how much is flowing through Tennessee.
States are getting pressure from clinicians ”who have had success with the use of ivermectin,” said IMA President Joseph Varon, a physician based in Houston. “That’s what happened in Texas, and that’s what happened in Tennessee.”
‘An Unproven, Potentially Unsafe Drug’
Once signed by Tennessee Gov. Bill Lee, the state’s ivermectin law took effect immediately — even before the state’s physician and pharmacy licensing boards created rules to guide the process, which Tennessee law also requires.
Some board members were shocked.
“We’re talking about an unproven, potentially unsafe drug,” Shant Garabedian, a doctor on the state’s Board of Osteopathic Examination, said of off-label ivermectin use during a 2022 meeting. “It’s already law. Somehow it passes without our sort of input.”
In meetings that followed, at least five members of Tennessee’s medical boards voiced concerns about the law beyond safety and efficacy. Some said pharmacists could overcharge for a drug that normally costs pennies per pill. Some worried that a loosely regulated, cash-based ivermectin market might attract shady characters, especially because the law also shields prescribers from ivermectin-related civil lawsuits.
“This involves no clinical engagement,” Melanie Blake, then-president of the Board of Medical Examiners, said during a 2022 meeting. “If they’re exempt from liability as well, I hate to think of things that individuals could do just to make money, but this would be one.”
Roman Pharmacy is one of the many compounding pharmacies in Tennessee that offer concentrated ivermectin pills. (Brett Kelman/KFF Health News)
The boards eventually enacted regulations affirming that ivermectin could be dispensed without any diagnosis. Board members said the law left them no choice.
“This is more of a situation where, legally, the legislature has decided for us,” John McGraw, another board member, said in a 2023 meeting. “This has sort of tied our hands in a lot of ways.”
The first known sale under the new law occurred in May 2022 in Sibley’s home of Johnson City, a city of about 74,000 people in northeastern Tennessee. According to a news release, Sibley entered into a collaborative agreement with pharmacist Josh Harrison at The Compounding Lab, which dispenses drugs for people and animals.
The first customer was Bernadette Pajer, an anti-vaccine activist who has worked with Children’s Health Defense. In a 2024 episode of the Nashville podcast Rebunked With Scott Armstrong, Pajer said Sibley was a medical adviser for the group and described the first ivermectin sale.
“On that day, she was the doctor, he was the pharmacist making the sale, and I was the first customer,” Pajer said. “So that was pretty cool.”
Ivermectin pharmacies have spread across the state. In the suburbs of Nashville, Roman Pharmacy advertises ivermectin on at least four billboards along Interstate 65, and its website is mostly focused on the drug. Outside Knoxville, Fresh Pharmacy allows customers to order ivermectin for multiple sclerosis and Parkinson’s disease, or “to use it to detoxify.”
Roman Pharmacy did not respond to interview requests. Fresh Pharmacy declined an interview.
In Chattanooga, the Medicine Counter pharmacy says on its website that ivermectin should be taken “only as prescribed by your healthcare provider.” And yet the pharmacy sells some of Tennessee’s most potent ivermectin available without a prescription from a doctor — up to 21 times as strong as a standard tablet, for nearly $19 per pill — according to the KFF Health News analysis.
Himanshu Patel, Medicine Counter’s head pharmacist, declined to be interviewed. He said in an email that the pharmacy operates in a “very competitive market” and that its strongest pills were below the maximum dose for humans evaluated by the FDA for safety purposes.
And then there is Compound Rx, which, in addition to selling ivermectin in its store, has built a website in preparation to ship buy-one-get-one-free pills nationwide. The site, which is in “test mode,” cannot currently make any sales. It also asks customers how they heard about the pharmacy, with a dropdown menu of answers that features right-wing figures such as Donald Trump Jr., Steve Bannon, Laura Ingraham, and Kevin Sorbo.
Who is not listed as an option? Your doctor.
Compound Rx, in Cookeville, Tennessee, is one of dozens of pharmacies in the Volunteer State that offer ivermectin without patient-specific prescriptions. Some pharmacies advertise the drug as available over the counter, even though customers technically have to request it from a pharmacist. (Brett Kelman/KFF Health News)
Hughey, the Compound Rx pharmacist, said he wasn’t involved with the website, which he said may never launch.
The highly concentrated pills are a concern for Tennessee state Sen. Richard Briggs, who worries lawmakers have created a “dangerous” ivermectin market rife with “misleading advertising” about what the drug can actually do.
Briggs, who is a surgeon and the only Republican who voted against the ivermectin bill in 2022, said he planned to introduce legislation to rein in the sale of ivermectin when lawmakers reconvene in 2027.
“But it may be a hard sell, because with the anti-vaxxers and some of these other folks,” Briggs said. “We don’t base a lot of things that we do on science, data, or facts. To a lot of folks in the legislature, the facts are just an inconvenience.”
‘Enough Trouble With Ivermectin’
Lawmakers in at least seven states have considered ivermectin legislation this year, including Alabama, Florida, Oklahoma, and South Carolina. If enacted, these bills would allow people to obtain ivermectin without an individual prescription, like in Tennessee, or make it available over the counter.
Kennedy praised such legislation at an event in Texas last August.
“I think it’s a really good bill,” he said of Texas’ ivermectin legislation, according to The Texas Tribune. “I think Americans should have the choice.”
But proponents have hit roadblocks. A Utah bill failed to advance out of the state House this year. In Oklahoma, some lawmakers have put up a fight.
“I’m a scientific person. I need to see some research and some data that shows what we’re treating,” Oklahoma state Rep. Cynthia Roe, a Republican and nurse practitioner who opposes the state’s ivermectin bill, said in an interview. “And God forbid somebody start giving it to their kid.”
Back in Tennessee, one of the medical boards that was alarmed when the law was enacted in 2022 started to distance itself from ivermectin altogether.
In January, the Board of Medical Examiners grappled with how to punish Ricky Lee Jackson, a doctor who was licensed in Tennessee and had been sanctioned and fined by Washington state’s medical commission. The Tennessee board normally mirrors punishments from other states without hesitation. But the Washington case centered on Jackson prescribing ivermectin for covid, which in Tennessee no longer required a patient to see a doctor.
After a debate, the board voted to reprimand Jackson — but told its staff to ensure the public record made no mention of ivermectin.
“This board has been in enough trouble with ivermectin,” member Keith Anderson said, according to a meeting recording. “Maybe we ought to just leave that out.”
In Maine, state health officials hoped to steer a slice of $190 million in new federal rural health funding to shield hospitals and clinics from the fallout caused by cuts to federal health programs.
Their plan would have helped pay to treat low-income, uninsured patients.
But federal leaders overseeing the five-year, $50 billion Rural Health Transformation Program said no.
“It was not our decision,” said Lisa Letourneau, a senior adviser at Maine’s health department.
Letourneau told an audience of healthcare providers, advocates, and community groups during a March webinar that the change was “disappointing.”
Maine isn’t alone in having to make changes to plans pitched to win a share of the Trump administration’s new rural health fund.
Centers for Medicare & Medicaid Services Administrator Mehmet Oz praised states’ plans when announcing the rural health program awards last year and said his agency would help states “turn their ideas into lasting improvements for rural families.”
But state officials and healthcare leaders said it’s also clear the agency wants to encourage specific policy changes and hold states accountable to the promises they made and rules they agreed to follow.
Email Sign-Up
Subscribe to KFF Health News' free weekly newsletter, "The Week in Brief."
During the past six months, as states raced to meet the program’s looming federal deadlines, CMS staffers worked with state health departments to make a flurry of changes, including scrapping some initiatives. The federal agency has the power to rescind existing funding — or reduce future awards — if states don’t follow rules or meet their goals. “We will take the money back” if states “don’t abide by what they wrote, if they don’t do a good job,” Oz said at an event this month in Washington, D.C.
Congressional Republicans created the Rural Health Transformation Program as a last-minute sweetener in their One Big Beautiful Bill Act last summer. The funding was intended to offset concerns about the outsize fallout anticipated in rural communities from the law, which is expected to reduce Medicaid spending by more than $900 billion over a decade.
Read an excerpt from the One Big Beautiful Bill Act.
MISUSE OF FUNDS.—If the Administrator determines that a State is not using amounts allotted or redistributed to the State under this subsection in a manner consistent with the description provided by the State in its application approved under paragraph (2), the Administrator may withhold payments to, or reduce payments to, or recover previous payments from, the State under this subsection as the Administrator deems appropriate, and any amounts so withheld, or that remain after any such reduction, or so recovered, shall be returned to the Treasury of the United States.
On a call with reporters in December, Oz said “one of the smartest things the president and Congress” did when creating the program was to create a threat of “clawbacks,” or taking money back if states don’t do what they promised in their applications.
Oz went on to describe how the clawback mechanism gives governors leverage to press their legislatures to adopt the Trump administration’s priorities, such as instituting the presidential fitness test in schools.
“This gives you extra umph, a little bit of gusto to go after these issues,” he said.
That message was received loudly and clearly in Tennessee. Michael Hendrix, policy director for the governor’s office, said during a hearing that federal officials said the state “would be more competitive for more funding through policy change.” He said CMS also relayed that “some share of this year’s funding, if policies are not implemented, might be clawed back.”
The threat of rescinding funding has caused fear and confusion among health organization leaders, said Alan Morgan, CEO of the National Rural Health Association.
“We’re worried that facilities and organizations won’t apply for the grant money because of the fears of the clawbacks,” he said, adding that he would like the administration to clarify if federal officials could take back grant money that states have already awarded to rural health organizations.
While clawbacks are a “necessary, important tool” to address misuse of funds and ensure the money goes toward helping rural communities, they are also “a dangerous tool,” said Morgan, whose organization represents rural hospitals and clinics.
CMS did not respond to multiple requests for comment.
States must file progress reports by the end of August. They then have until Oct. 30 to commit their first-year funding and Sept. 30, 2027, to spend it.
States are progressing at wildly different rates, with some still developing grant applications and others already distributing money, according to a tracker created by Morgan’s rural health association.
In late January, Iowa became the first to award funding. The tracker shows that most states have opened grant applications, but 11 others, including Wyoming, Maine, and Colorado, have yet to post any funding opportunities.
CMS’ tight control over state programs is one reason for such disparity in progress.
Instead of typical grants, the rural health program uses cooperative agreements, which require a back-and-forth partnership, said Charlie Sagona, a grant specialist at Assel Grant Services, a consulting firm that helps organizations manage grants.
“You are going to be working very, very closely with them; things will ebb and flow and change and move,” said Sagona, who is helping several large hospital systems interested in winning some of the rural funding.
Kate Sapra, deputy director of CMS’ Office of Rural Health Transformation, said at a May event that the agency has “many avenues of oversight.” Staffers are tracking applications for state funding and “looking to see when contracts are executed,” she said.
Sapra said the agency wants to “have conversations with states before they get to the point” of putting out something that’s not allowed. It’s “really important to us” for the funding to reach rural providers, she added.
Sapra said her office has filled about half of 30 new slots for project officers. The officers and the states check in “at least twice a month, if not on a weekly basis.”
Vermont Medicaid Director Jill Mazza Olson, who led her state’s rural health application, said the officers are “very responsive.”
Vermont is one of the states that had to ditch or tweak its plans. Olson said the state pulled its plan to increase housing for rural healthcare workers after federal officials said they would evaluate the proposal based on the agency’s guidelines for construction projects at healthcare facilities. Those rules allow only “minor” renovations to existing buildings or campuses.
In Colorado, state leaders changed grant eligibility rules after they “received feedback” from CMS and healthcare providers, said Marc Williams, a spokesperson for the state’s Department of Health Care Policy and Financing.
Wyoming legislators and state officials spent months designing, discussing, and voting on a plan to invest most of its award into a perpetuity fund that could have generated $28.5 million for the state to spend every year, “forever,” according to materials presented to lawmakers.
The state had to pull the idea because it “was a degree too innovative for CMS to swallow,” said Republican state Sen. Charles Scott, a veteran lawmaker and cattle rancher. “This whole thing has been a bit of a disappointment to us in Wyoming.”
Stefan Johansson, director of the state’s health department, said Wyoming’s final spending plan wasn’t approved until mid- to late May. He said the department hopes to begin awarding money in late summer or early fall.
“Make no mistake — it is a very compressed timeline,” he said.
Across the country, Maine was forced to rework its plan to reimburse hospitals and clinics when they provide “essential” care to certain uninsured patients.
Letourneau said during her March remarks that federal officials rejected this idea because “provider payments had to be more directly linked to a rural transformation kind of activity.”
Lindsay Hammes, a spokesperson for Maine’s health department, told KFF Health News that funding will instead help providers transition to reimbursement models that aren’t based on how many patients they treat.
Reworked plans call for spending $28.5 million to support providers, Letourneau said in March.
“But there definitely will be more strings attached.”
KFF Health News correspondent Darius Tahir contributed to this report.
Early-Onset Cancers Are on the Rise. Knowing Your Family History Is Crucial.
Listen in and play along as hosts Cara Anthony and Blake Farmer test their knowledge with a HealthQ quiz on detecting early-onset cancers.
(Candice Evers for WPLN and KFF Health News)
Bryce Ramsey of Madison, Mississippi, was 33 when she was diagnosed with colorectal cancer. Upon noticing blood in her stool, she blamed the hemorrhoids she’d developed after delivering her son eight years earlier.
Ramsey didn’t initially link her symptoms to cancer.
“But I had just kind of made a deal with myself because the blood was starting to become more frequent,” she said. “I was like, ‘If this happens the next time I go to the bathroom, I’m going to make a call.’”
She saw more blood, and she reached out to a gastrointestinal clinic to get it checked out, just in case. Her doctor said she normally wouldn’t scope someone Ramsey’s age, “‘but something in my gut is just telling me I need to do so,’” Ramsey recalled. “And thank God she did because she found a 5-centimeter polyp.”
Ramsey had surgery, endured chemotherapy, and survived stage 3 colon cancer. Now 40, she volunteers for the Colorectal Cancer Alliance, a nonprofit advocacy group, to raise awareness of early-onset colorectal cancer.
Stories like hers are becoming increasingly common: In the U.S., more than a dozen kinds of cancer are on the rise in adults under 50. Among these early-onset cancers, colorectal and breast cancers have increased the most, and colorectal cancer is now the deadliest cancer for Americans ages 18 to 49.
Here’s what to know about detecting early-onset cancers.
1.Family history is one of the most important risk factors.
Researchers have not been able to find a single cause for the rise in early-onset cancers. Instead, research suggests a myriad of factors play a role, including obesity, heavy alcohol use, environmental factors such as microplastics, and disruptions to gut health.
Doctors generally follow population-level guidelines for routine screenings — such as recommending mammograms starting at age 40 to screen for breast cancer — but physicians might recommend some patients get screenings as early as in their 20s. Doctors weigh a patient’s personal risks, including their family history of cancer.
Ramsey learned only after her diagnosis that her grandfather previously had colorectal cancer. “If I would’ve known that I had a significant family history, I would’ve been scoped a lot younger,” she said. “My doctor said my tumor had probably been growing for seven to 10 years.”
After her diagnosis, she encouraged her father, aunt, and brother to get screened. All three were diagnosed with colon cancer, too, and survived after receiving treatment.
Ramsey said it can be uncomfortable to urge family members to get tested or to talk with them about private health information, but those conversations are worth having to save a life.
“Just ask the question or make a joke about it. And sometimes just little icebreakers will help,” she said.
Email Sign-Up
Subscribe to KFF Health News' free Morning Briefing.
2.Report unusual symptoms as quickly as possible.
Being vigilant about unusual body changes or symptoms — and reporting those to your physician — gives doctors the information they need to determine your personal risk for cancer.
“For example, a lump in the breast, abdominal pain, changes in bowel habits that really are not going away,” said oncologist Veda Giri, director of the Early Onset Cancer Program at Yale Cancer Center. “Certainly blood in the stools. Sometimes even symptoms such as unusual fatigue that doesn’t seem to go away.”
“It’s incredibly important to bring symptoms to your doctor,” Giri said.
3. Talk, then test, then talk again.
Ads for at-home cancer tests are everywhere, so you might be tempted to use a screening kit instead of going in for an office visit or a standard screening, like a colonoscopy.
But not all tests are created equal, Giri said. It can be hard for laypeople to understand the accuracy of at-home screening kits, so they should talk to their doctor first.
“Some of these tests could lead to a false sense of either reassurance or false anxiety and alarm,” she said.
For people who decide to move forward with an at-home test, experts say they still need to consult with a physician. If you get any sort of abnormal result, your doctor is going to want to follow up with additional testing, such as a colonoscopy. Sharing your results, regardless of outcome, will help inform your care.
People and Policy
The U.S. Preventive Services Task Force recently changed the recommended age for women to begin mammogram screenings for breast cancer from 50 to 40. But there’s a difference of opinion among national advocacy and medical groups about whether regular screenings should happen every year or every other year.
In 2021, the same task force lowered the recommended age to 45 for a first colonoscopy for colon cancer detection for people with average risk. Establishing a relationship with a trusted medical practitioner can help patients assess personal risk and sort through new information as research and public health guidance evolve.
If you feel uncertain about your personal risk for cancer or when you should start cancer screenings, one of the best ways to advocate for your health is to establish a relationship with a medical practitioner you trust and ask specifically about your cancer risk. You can also ask to consult with a genetic cancer risk specialist, a type of medical provider who helps patients evaluate their cancer risk, often with genetic testing.
This installment is part of HealthQ’s reporting on caregiving among the sandwich generation. For more, check out the series archive.
Katherine Ruppelt and Emily Siner at Nashville Public Radio contributed to this report.
HealthQ is a health series from reporters Cara Anthony and Blake Farmer, approachable guides to an unapproachable healthcare system. It’s a collaboration between Nashville Public Radio and KFF Health News.
Long-Awaited Rule Aims To Boost ACA Choices While Embracing Higher Deductibles
Long-Awaited Rule Aims To Boost ACA Choices While Embracing Higher Deductibles
The Affordable Care Act seems to always be in a policy tug-of-war as its backers and critics spar over how it should work and who can qualify for coverage. This year is no different, with the Trump administration embracing standards it says will reduce fraud as well as steps that could further erode national enrollment.
Wide-ranging ACA changes pushed by the administration were finalized in mid-May, including new offerings such as plans with 30% higher out-of-pocket costs, and others with no set networks of doctors and hospitals.
The administration says such plans expand consumers’ choices and may carry lower premiums.
The rule stated, though, that the combined effect of the new provisions could not only cost $1.3 billion each year to implement, but also reduce enrollment by up to an additional 2 million next year. That would come on top of already anticipated sign-up decreases this year because of higher premiums and smaller subsidy payments.
Over time, lower enrollment can boost premiums if insurers suspect their costs are rising because healthier people drop coverage more than sicker members do.
Some policy experts fear the changes will erode the ACA and make it more expensive, particularly for those whose subsidies have shrunk or disappeared.
“Even more people will lose coverage as healthcare costs and administrative burdens rise,” said Katie Keith, director of the Center for Health Policy and the Law at the Georgetown University Law Center, who writes frequently on changes to the ACA. “All of this comes at a time when millions of consumers are already experiencing a healthcare affordability crisis.”
The lengthy payment rule is an annual exercise in which the Centers for Medicare & Medicaid Services, which oversees the ACA, can set new standards for coverage. The rule for next year is more ambitious than in past years, with changes to how plans are designed, eligibility verification, and adjustments needed to implement congressional legislation, along with technical updates.
Here are some of its biggest changes.
Non-Network Plans
Starting in 2028, some Affordable Care Act consumers may be able to pick plans that don’t have dedicated networks of doctors and hospitals, which patients use to qualify for negotiated in-network payment rates.
Under this new model, enrollees would seek out providers willing to accept the amount their insurer will pay toward whatever nonemergency care they need, such as a sore throat, a doctor visit, or childbirth.
The rule requires insurers to have “a sufficient choice of providers that accept the non-network plan’s benefit amount as payment in full.”
Regulators say the policy aims to reduce costs by getting consumers to “shop for lower prices and negotiate directly with providers.”
Email Sign-Up
Subscribe to KFF Health News' free Morning Briefing.
But how the plans will work — and how they will be monitored for having enough practitioners — isn’t yet clear, and that has raised concerns with some experts who say non-network plans might chip away at ACA safeguards intended to ensure enough medical providers are available in a given area. Patients could also find themselves on the hook financially when they find their doctor or hospital charges more than the insurer will reimburse.
Economist Matthew Fiedler, a senior fellow at the Brookings Institution, pointed out another potential pitfall with this approach.
“It may not always be obvious whether enough providers are willing to accept the plan’s rates,” he wrote in a comment letter to regulators. “If this is the case, non-network plans likely would offer lower premiums, mainly by paying lower prices for care and making accessing care harder.”
There will likely be variation by state in how such plans must prove they have an adequate number of care providers willing to accept amounts as payment in full, said Louise Norris, a health policy analyst for healthinsurance.org, a consumer information and referral website affiliated with Trove Group.
“I would put a big buyer-beware notice on non-network plans,” she told KFF Health News. “Consumers will need an understanding of how this will work, and also it puts the onus on the consumer to find out what the provider is charging.”
But other viewpoints, including from the Paragon Health Institute, a conservative think tank, consider the non-network plans a step forward for transparency and competition because they empower consumers.
“When consumers can see what the plan will pay and how provider prices vary, they have incentives to shop,” noted Paragon’s comment letter.
It will take time and more federal guidance, though, before it becomes clear what additional requirements these plans will face and how many insurers will decide to offer them. Some clues can be found in non-network plans sold by Ohio-based Sidecar Health, which offers such coverage in Ohio, Florida, Georgia, and Texas with enrollees in 48 states — but only for employer plans.
Click to read more about how this kind of coverage works
Non-Network Plans: A Real-Life Example
Ohio-based Sidecar Health offers a non-network health plan with a glimpse into how the Trump administration’s proposal might function when such plans become part of the Affordable Care Act marketplace in 2028.
For now, the plan is available only to people who get coverage through their jobs.
The company’s chief marketing officer, Kevin Knight, said members have access to an app and the company’s website, which displays estimated costs of healthcare across a range of treatments and practitioners in a given area.
Sidecar also allots benefit amounts to members for covering their care, aiming to set them at levels of at least 50% of what providers in a region are already being paid, usually by other commercial insurers.
For nonemergency care, enrollees choose a provider, often after checking their benefit amount. Enrollees usually pay in full — using a Sidecar credit card or their own — at the time of their visit. They then submit an itemized invoice, clinical notes, or other data to Sidecar.
If the doctor, hospital, or clinic the enrollee chooses costs more than the benefit amount, the patient pays the difference. If the care costs less, they get money back from Sidecar, which estimates the average member earns $250 annually by choosing providers with lower costs.
Emergency care is handled differently, with payments made by Sidecar directly to the hospital. Because of the No Surprises Act, enrollees wouldn’t face additional costs. That measure prevents hospitals from billing patients for amounts above what their insurer pays when they need out-of-network emergency care.
Sidecar gets mixed reviews on sites like Trustpilot and the Better Business Bureau. Some customers praise the insurer, saying they like being more in control of their choice of doctors, while others report dissatisfaction over the claims process.
Knight said many of the concerns on such online websites preceded the rollout of an updated app last year that incorporates the benefit amounts.
Still, some health policy analysts say there are many reasons for consumers to proceed with caution, both in the employer market and when these plans become part of the ACA offerings. Among the issues they cite are concerns that an adequate number of providers will participate or that consumers’ finances will be exposed.
Higher Out-of-Pocket Costs
Another change coming soon is the potential for higher ACA out-of-pocket costs.
Under the final rule, insurers can set higher maximum out-of-pocket limits in two types of plans: bronze and catastrophic. That begins in 2027 for bronze plans, which already have the highest annual deductibles of all the metal-tiered plans but generally lower premiums as a result.
Starting next year, any insurer that offers at least one bronze plan with a regular out-of-pocket maximum — the total amount a consumer is responsible for in copayments and deductibles during the year — can also offer one that has up to a 30% higher maximum than otherwise allowed.
That means some bronze plan out-of-pocket maximums could be $15,600 for individual coverage or $31,200 for a family plan.
Regulators say they need to set these criteria because bronze plans increasingly can’t meet other ACA requirements without increasing those limits. Federal regulators admit the higher amounts could result in “financial challenges for some enrollees” because they might not have enough in savings to cover those costs, according to an analysis of the new rules by Keith at Georgetown.
And here’s another change: Starting in 2028, insurers offering catastrophic plans, which are available for people age 30 and under as well as people who don’t qualify for premium subsidies, will see 30% higher out-of-pocket maximums.
The thresholds may be similar to what some bronze plans offer, but there are differences. Catastrophic plans must be set at the higher levels; it’s not optional. And, in those plans, nothing except preventive services and up to three primary care visits are covered before the consumer must meet the new higher deductible amounts, the point at which insurance will kick in. Consumers cannot receive ACA subsidies to help them purchase a catastrophic plan.
While the premiums may be lower, it isn’t clear whether such plans will attract substantial numbers of enrollees, even with lower premiums. To balance the lower premiums against the higher potential out-of-pocket costs, enrollees will need to gamble that they will remain healthy or have access to savings to cover costs. Data shows that many Americans have limited savings, with median balances ranging from $5,400 to $8,700, well below thresholds in catastrophic plans.
Beginning next year, insurers will be allowed to sell catastrophic plans that could remain in effect for years, rather than renewing annually.
The combination of the higher out-of-pocket costs, along with other legislative changes, and the increased paperwork requirements is “not ending Obamacare as we know it,” Keith said, “but will significantly erode access to the marketplaces. Fewer people will benefit.”
A few other changes are listed in the rule, some of which stem from the tax and spending bill Congress passed last year known as the One Big Beautiful Bill Act.
The measure makes permanent a previous decision to halt a special enrollment period that allowed very low-income people to sign up for ACA coverage year-round. Backers, including Paragon, say this can help cut down on fraudulent enrollments.
The new rule would put in place additional income verification requirements, including for people who say their income is above the poverty level and thus qualify for subsidies, despite federal data indicating their income might be below the poverty level.
In addition, it would require more checks on people applying for special enrollment periods — such as for loss of job-based coverage or for marriage or divorce — seeking information that they qualify. Also, premium tax credits would be denied to people who have not filed their taxes for one year, down from the current two.
“Unless this gets blocked by another court case, consumers will have to provide more documentation for special enrollment eligibility verification,” Norris said.
“If they get married and want to add a spouse, for example, they’ll have to provide a copy of the marriage license,” she said. “Those factors will definitely depress enrollment because it will be more hurdles for people to jump through, but CMS also says it will save money on subsidies.”
They’re Uninsured After Obamacare Became Too Costly. And They’re Far From Alone.
They’re Uninsured After Obamacare Became Too Costly. And They’re Far From Alone.
Some families have decided the price is too great of a financial burden and canceled their coverage.
Rebecca and Ross Tobiassen, who own an auto shop in the North Carolina mountains, canceled their Affordable Care Act insurance last year when it became too expensive. (Andrew Jones/KFF Health News)
SUGAR GROVE, N.C. — Year after year, Ross and Rebecca Tobiassen saw their healthcare costs rise, having relied on the Affordable Care Act for federally subsidized health insurance since its start in 2014. Year after year, the couple in western North Carolina kept their coverage, believing the peace of mind was worth the cost.
But in December, that changed. The Tobiassens decided to cancel their insurance when Rebecca saw the cost of their monthly premiums would jump from $130 to more than $550.
“It makes no sense,” she said. “It’s not worth it anymore.”
The couple own and are the only employees of a small auto shop just west of Appalachian State University in the North Carolina mountains. Rebecca worries about her husband, whose work as a mechanic can be dangerous. A spring once shot a metal ball joint into their garage wall like a gun. A heavy object crushed Ross’ thumb. In 2020, Ross became mostly blind in one eye after repeatedly getting metal shards in it and developing an infection in his cornea.
The Tobiassens are among the Americans who canceled their ACA coverage after Congress allowed enhanced tax credits that helped pay for insurance plans to expire at the end of 2025. The Tobiassens benefited from those tax credits — like millions of other enrollees expected to drop or be dropped from their coverage as the year progresses, unable to keep up with the higher costs.
Established by the Biden administration’s American Rescue Plan Act during the covid pandemic, the expanded subsidies reduced monthly premiums for many families and prompted a tidal wave of new sign-ups, doubling ACA enrollment to about 24 million.
The Centers for Medicare & Medicaid Services is expected to soon release complete data on how many people are no longer covered under the ACA, but an early analysis from KFF, citing Wakely Consulting Group research, showed enrollment could drop from over 22 million at the end of 2025 to as low as 16.5 million in 2026.
In North Carolina, individual ACA sign-ups for 2026 were down 22% compared with the year before, a greater drop than any other state, amounting to a decrease of more than 213,000 people, according to enrollment data. While the Tobiassens’ two teenage daughters remain on Medicaid, Rebecca said the new prices showed that the federal government doesn’t care about families like hers.
“We’ve known that you don’t care about us,” she said, “but you’re making it plain and simple now.”
Ross Tobiassen became mostly blind in his left eye after repeatedly getting metal shards in it while at work in his auto shop and developing an infection in the cornea. (Andrew Jones/KFF Health News)
The couple’s insurance hadn’t helped them cover all their medical needs. When the pain from Ross’ eye infection worsened five years ago, Rebecca insisted he go to a specialist, who told them that fixing the eye through cornea replacement surgery would cost them up to $30,000 and require Ross to take six months off.
Ross chose a less expensive treatment to kill nerves in the eye instead.
The couple know they’re taking a risk by not being insured. If something were to happen, they could face an enormous medical bill.
Ross, 47, said the blindness in the one eye doesn’t significantly affect his job. He works long hours, sometimes into the night to keep up with demand.
“I try not to think about it too much,” he said. “I just work.”
Email Sign-Up
Subscribe to KFF Health News' free Morning Briefing.
Uninsured, With No Backup Plan, After Obamacare Became Unaffordable
Rebecca Tobiassen, 44 Sugar Grove, North Carolina
Rebecca Tobiassen owns a small auto repair shop with her husband, Ross, in the western North Carolina mountains. She says their family could no longer afford Affordable Care Act insurance after tax credits expired last year and their monthly premiums shot up from $130 to more than $550. They have no immediate plans to sign up for coverage elsewhere and are saving up for out-of-pocket expenses instead. “We just need to be able to afford to get help when we seriously hurt ourselves,” she said of the U.S. healthcare system.
Katie Alexander oversees volunteers for Pisgah Legal Services, a western North Carolina nonprofit that helps low-income people secure health insurance. Alexander has helped North Carolina and Tennessee residents try to get ACA marketplace plans since Obamacare’s launch. She said she’s never seen anything like this year.
Nearly 100 Pisgah clients, out of about 700 that Alexander’s team worked with during open enrollment, decided to drop insurance this year, and many others chose cheaper ACA plans with less coverage, Alexander said.
Alexander said the people who have dropped their coverage include Lyft and Uber drivers. They’re trying to start their own businesses. They are artists and people who can work only part-time, because they’re chronically ill. Some are unable to get insurance through their employers, or they make too much to be on Medicaid.
“Even for folks who don’t have chronic illnesses,” Alexander said, “there’s just this nagging at the back of your mind, kind of constantly, of: ‘Don’t get hurt. Don’t get sick. Because you can’t afford that.’”
ACA premiums and deductibles steadily increased for years starting in 2022, then spiked during the enrollment period for 2026 plans, according to data analyzed by KFF. The Tobiassens have seen every dip and rise in plan costs since 2014 when the plans launched. They joined immediately and paid about $30 a month, Rebecca Tobiassen said.
“You actually felt like you were benefiting,” she said.
But through the years as the marketplace became more expensive, the couple made concessions, switching at one point from a silver plan — historically the most popular — to a bronze. The plan mostly provided for the couple’s basic needs.
As they saw their deductibles and premiums rise over more than a decade, Rebecca feared the day would come when they could no longer afford even the cheapest plan.
“Plans are unaffordable, no matter how you cut it,” said Risha Gidwani, a healthcare policy researcher at the University of Colorado Anschutz School of Medicine. “It’s just who is shouldering the unaffordability.”
Ross Tobiassen built his auto shop, which he owns with his wife, next to his home on his property in western North Carolina. (Andrew Jones/KFF Health News)
Ross Tobiassen says his job as a mechanic can be dangerous — he works late into the evenings sometimes to keep up with demand. (Andrew Jones/KFF Health News)
Gidwani and health economist Cheryl Damberg, in a study published earlier this year, found that most bronze plans, the cheapest ACA options for many, would be unaffordable without subsidies for the average person using the federal healthcare coverage.
Without subsidies, many families using these plans don’t make enough to afford premiums or deductibles, Gidwani’s research shows.
People who drop health insurance also change what’s known as the “risk pool,” Gidwani said, when a group of people share financial hazards.
If healthier people drop out of the risk pool, fewer people subsidize the people who get sick, Gidwani said. That means premiums for the people who get sick will increase again in the future, she added.
“That becomes what we call a death spiral,” Gidwani said.
Even if the subsidies hadn’t expired, taxpayers would have borne an estimated $350 billion burden over the next decade to cover them, Gidwani’s study noted.
After dropping coverage they’d relied on for 11 years, the Tobiassens have no plans to return to the ACA marketplace. They looked into alternative options through a faith-based healthcare organization but decided to go without.
For now, they don’t have a plan B. They’ve set aside some money for a medical emergency. And if their savings run out, Rebecca Tobiassen said, they have a couple of last resorts to lean on: credit cards or family members.
Are you struggling to afford your health insurance? Have you decided to forgo coverage? Click here to contact KFF Health News and share your story.
Journalists Highlight Medical Neglect in ICE Detention, RFK Jr. Antidepressant Comments
Journalists Highlight Medical Neglect in ICE Detention, RFK Jr. Antidepressant Comments
June 13, 2026
KFF Health News chief Washington correspondent Julie Rovner discussed Health and Human Services Secretary Robert F. Kennedy Jr.’s position on antidepressants on WAMU’s 1A on June 10.
KFF Health News journalist Rae Ellen Bichell discussed, on WBUR’s Here & Now on June 10, a recent investigation that found immigration facilities aren’t providing adequate medical care.
KFF Health News national public health correspondent Amy Maxmen discussed the Ebola outbreak in the Democratic Republic of Congo on WNYC’s The Brian Lehrer Show on June 9.
Céline Gounder, KFF Health News’ editor-at-large for public health, discussed on Fox’s LiveNow on June 8 how public health experts are preparing for the World Cup.
Elisabeth Rosenthal, KFF Health News’ senior contributing editor for health news analysis and author of the bestseller An American Sickness: How Healthcare Became Big Business and How You Can Take It Back, discussed the challenges of reforming the American healthcare system on NBC’s Dateline on June 5.
The issue of affordability has reignited a long-simmering battle between California’s medical industry and one of its largest health worker unions.
SEIU-United Healthcare Workers West, with approximately 120,000 members, has put forward two ballot initiatives to cap the pay of medical executives and require community clinics to spend the vast bulk of their revenues on patient care.
The California Hospital Association has responded with its own ballot proposal that would make it tougher for unions to spend money on future political initiatives by requiring a union’s rank-and-file membership to approve any spending of at least $1 million on statewide measures or $100,000 on local ones.
The competing measures, which have drawn enough verified signatures to qualify for the November ballot, come at a time when the rising cost of healthcare is emerging as a top voter concern.
Email Sign-Up
Subscribe to KFF Health News' free weekly newsletter, "The Week in Brief."
The Service Employees International Union affiliate has seized upon affordability angst to resurrect failed proposals to cap healthcare executive compensation.
Mikey Vaughn, a certified nursing assistant at Cedars-Sinai Medical Center, said that the Los Angeles hospital, despite its reputation as the go-to place for the rich and famous, often lacks supplies and staffing that he and his colleagues need to do their jobs.
But that’s not how hospital officials see it. Cedars-Sinai spokesperson Duke Helfand said if the measure passed, the hospital would be unable to recruit and retain physicians, nurses, and specialists, dramatically impairing its ability to provide healthcare.
The union wants to cap compensation at $450,000 a year for senior hospital and medical group executives, as well as other administrative and managerial staff. SEIU-UHW does not have an estimate of the amount the initiative would claw back from pay packages that exceed the limit. And the initiative does not stipulate how dollars diverted from payroll must be spent.
Carmela Coyle, CEO of the hospital association, called the measure a cynical political ploy.
And Glenn Melnick, a healthcare economist at the University of Southern California, said that even if the initiative were fully implemented, he doubts it would reduce patients’ healthcare costs.
The second SEIU-UHW ballot initiative, on community clinics, is already in court. The California Primary Care Association, which represents clinics, filed a federal lawsuit in April seeking to invalidate it before it reaches the November ballot.
One of California’s largest healthcare unions is sponsoring two initiatives that would regulate community clinics and cap executive and managerial pay at hospitals and physician groups. In the most recent eruption of a long-standing feud, the measures have drawn fierce opposition from a wide swath of the medical industry.
Centers for Medicare & Medicaid Services Administrator Mehmet Oz. (David Berding/Getty Images)
The Trump administration has issued final rules on how states should ensure that millions of Medicaid enrollees prove they’re working or completing other activities, such as job training, volunteering, or being enrolled in an educational program.
The Centers for Medicare & Medicaid Services released the rules on June 1. That deadline was set last year in the GOP tax-and-spending law known as the One Big Beautiful Bill Act, which established a work requirement for certain people enrolled in Medicaid, the state-federal health insurance program for people with low incomes or disabilities.
Medicaid agencies are scrambling to rework IT systems and make sure they have staff to effectively enforce the rules, while also keeping enrollees from losing coverage for administrative reasons, such as difficulty navigating state eligibility portals.
The newly announced regulations offer a clearer picture of what roughly 18.5 million Medicaid enrollees will have to do to prove they qualify for benefits.
Email Sign-Up
Subscribe to KFF Health News' free weekly newsletter, "The Week in Brief."
Jim Torres, who helps people enroll in health coverage at the Samuel U. Rodgers Health Center in Kansas City, Missouri, said a “very small percentage” of his clients have heard of the changes coming to Medicaid.
“These folks have very busy lives. They’re doing the best they can to get by,” he said. “It’s just not a top-of-mind thing for most of them.”
Health policy researchers and consumer advocates said enrollees should keep a few things in mind as the Jan. 1, 2027, rollout approaches in most states.
1. The work rules won’t apply to everyone.
The new rules will apply to people covered through what’s known as Medicaid expansion. Since 2014, more than 40 states and the District of Columbia have decided to allow more people into their Medicaid programs, generally low-income adults without dependents. Georgia and Wisconsin offer coverage to some people in this group, so they’ll be subject to the rules.
Children and pregnant people, as well as individuals with disabilities who receive Social Security payments — all groups that already qualify for Medicaid — won’t be subject to the rules. Nor will people determined to be “medically frail,” or too sick to work.
People subject to the work rules are “crowding out” people in the Medicaid program who are “truly in need,” CMS Administrator Mehmet Oz claimed during a June 1 press call. “Work requirements are going to turn this around, we hope.”
2. States will take your word that you’re too sick to work. For now.
Federal officials have stressed that states should make the process of reporting hours and requesting exemptions as simple as possible for Medicaid enrollees by creating automated systems and using existing data sources, such as unemployment and education records.
If states cannot determine you’re performing 80 hours of qualifying activities a month using those data sources, you may be allowed to “self-attest” to that in 2027, health policy researchers said.
People will also be allowed to “self-attest” that they are too sick to work in 2027, and do so one time in 2028. Then states will start asking for proof, if they can’t find it through available data.
But after the initial rollout, the burden of proof is likely to still fall on many enrollees, said researchers and consumer advocates.
People may need to dig up pay stubs, medical records, and doctors’ notes and submit them for state review, said Morgan Henderson, who has studied Medicaid work programs in Georgia and Arkansas at The Hilltop Institute, a research center at the University of Maryland-Baltimore County.
“The higher this manual reporting burden, the less people are going to do it,” he said. “That means that we’re going to see coverage drop-offs.”
3. The rules are tougher than expected for people too sick to work.
One of CMS’ primary goals has been to “protect vulnerable populations” through “strong exemptions to make sure people who can’t reasonably be expected to work are not subject to the requirements,” Dan Brillman, a deputy administrator at the agency, said during the June 1 press call.
Consumer and patient advocates, however, said the final rules’ exemptions are more restrictive than expected. Enrollees will eventually have to provide documentation, such as a statement from a medical professional, to prove that a health condition keeps them from working. And each individual state will have to determine the severity of beneficiaries’ medical conditions.
“Someone could be medically frail in Nebraska but not medically frail in Delaware,” said Carolyn Sheridan, associate director of state policy for the National Organization for Rare Disorders, which lobbies for patients with rare diseases. She said her group had hoped the rules would offer a standardized definition of who counted as medically frail and not leave the decision up to states.
Trump administration officials have publicly crusaded against fraud in government health programs, such as Medicaid, and states could face financial penalties for incorrectly granting people exemptions from the work rules, said Jennifer Tolbert, who researches Medicaid at KFF, a health information nonprofit that includes KFF Health News.
“States may be more cautious,” she said. “That will likely lead to people losing coverage who may still be eligible.”
4. Only certain qualifying activities count.
Enrollees can satisfy the rules by working 80 hours a month. They can also be enrolled in college courses, volunteer through a community organization, or do “in-kind” work that doesn’t result in pay.
The rules set out, in detail, how many academic credit hours translate to 80 hours a month — students need to be enrolled in six credit hours per semester to meet the “half-time” requirement. An unpaid internship can count toward the 80 hours.
People can also prove they’re volunteering with “a document from a community service organization.”
Consumer advocates say it might be hard for people to obtain proof they’re performing these kinds of informal activities. But supporters of the rules say volunteerism can already be tracked.
“If you run into trouble with the law and the judge says, ‘Hey, you need some volunteering and community service to serve your time,’ there are already ways that we verify that,” said Niklas Kleinworth, who works on state health policy for the conservative Paragon Institute.
5. You have time to prepare.
Make sure your state Medicaid agency has your current mailing address and keep your eye on your mailbox, said researchers and consumer advocates. State Medicaid agencies must inform you in two ways if you’ll be subject to the rules — by either regular mail or email, and by one other form of communication, such as a text or phone call or by posting a notice online.
“The important stuff comes by mail,” Henderson said.
And check in with your state Medicaid agency, said researchers and advocates. Some states, including Arkansas, California, and Wisconsin, have already posted information about the work rules on their websites. If you can’t find what you’re looking for there, visit or call a local office. A caseworker should be able to tell you whether you’ll be subject to the rules.
“Get ahead of this,” said Joan Alker, who is executive director of the Georgetown University Center for Children and Families and studies Medicaid. “So that you don’t end up going to the pharmacy one day and they say, ‘Oh, you’re not insured anymore’ when you’re trying to get your prescriptions refilled.”
KFF Health News correspondent Samantha Liss and senior correspondent Rachana Pradhan contributed to this report.
Have you tried to prove your eligibility for Medicaid under new rules that require people to show they are working, going to school, or participating in another qualifying activity? Click here to contact KFF Health News.
1 in 4 Covered California Enrollees Could Get State Aid Under Newsom Proposal
California Gov. Gavin Newsom delivers his final state budget plan in Sacramento on May 14. (Gabrielle Lurie/San Francisco Chronicle via Getty Images)
0:000:00
Speed
Embed this player
When Congress allowed covid-era subsidies for health insurance to expire, California used its own funds to offset the hike in Obamacare premium costs for residents with low incomes.
But the reach has been limited.
As Gov. Gavin Newsom negotiates his last budget with the legislature, the Democrat wants to offer financial help to more than 1 in 4 enrollees in Covered California, the nation’s largest state-run health insurance marketplace. Democratic lawmakers, who hold a supermajority, are still debating the plan.
“My budget proposal would KEEP $0 monthly plans for low-income Californians to help clean up the financial disaster Trump created,” Newsom posted on Facebook, where he often chides the president and GOP Congress.
Ten blue states have put up their own funds to keep Affordable Care Act plans affordable and residents insured as the rising cost of healthcare has emerged as a top concern among voters. Newsom’s $300 million proposal would make California’s program among the most generous, but even the nation’s richest state can’t patch a $2.5 billion hole left by the expiration of enhanced subsides at the end of last year.
“The gap between what people can pay in their monthly budget and what health insurance costs is so big that it’s a lot for states to take on,” said Stacey Pogue, a senior research fellow at the Center on Health Insurance Reforms at Georgetown University. “They’re going to have to figure out how they can finance that.”
Email Sign-Up
Subscribe to KFF Health News' free Morning Briefing.
New Mexico lawmakers have backfilled 100% of the lost federal subsidies with state money. It seems to have worked; New Mexico saw double-digit increases in marketplace enrollment this year, but state analysts have warned that the subsidy program isn’t sustainable.
Massachusetts and New Jersey, which, like California, tax residents for not having health insurance, are also spending hundreds of millions of dollars to try to keep premium payments low. Their hope, healthcare experts say, is to avoid the exodus seen in states such as Georgia that didn’t offer enrollees help.
Since the enhanced subsidies expired, enrollees nationwide have seen their premium payments increase by $65 a month on average.
“There are never enough subsidies to make health insurance affordable because subsidies are the problem,” said Michael Cannon, director of health policy studies at the libertarian Cato Institute. “They are causing people to turn a blind eye to fraud and waste and excessive prices because it’s someone else’s money that they’re spending, not their own.”
Helping the Poorest?
People who earn too much to qualify for Medicaid got relief starting in January after Newsom and legislators softened the blow for about 300,000 of the lowest-income enrollees. They offset lost federal premium tax credits for individuals who earned up to $23,475 last year and partially filled the gap for those who earned up to $25,823.
The governor now wants to expand subsidies to those who earn up to $31,920 this year for an individual and $66,000 for a family of four — an estimated 218,000 additional people.
Veronica and William Walter, who live in the San Francisco Bay Area, earn less than $40,000 a year in one of the nation’s most expensive regions. They’re counting on a more generous state healthcare tax credit if they have to pay for health insurance next year.
Veronica Walter says she wouldn’t be able to afford the nearly $200 monthly premium for health insurance that she and her husband would likely pay on Covered California, even after a proposed expansion of state subsidies. (Christine Mai-Duc/KFF Health News)
A car accident two years ago left William temporarily disabled, qualifying the couple for Medi-Cal, the state’s Medicaid program.
Now he’s back at work as a security guard, and Veronica said she’s worried they’ll be kicked off Medi-Cal. She’s even more worried about how they’ll get by with federal premium tax credits not nearly as generous as before.
“Without it, we’re going to be facing worse problems than we have now,” she said. Under Newsom’s proposal, Veronica and others in the highest eligible income bracket could receive an average monthly subsidy of $36 a person.
“For them, $36 a month is the sort of thing that can make a difference between keeping coverage and losing coverage,” said Peter Lee, former executive director of Covered California. “We can’t fix everything with that gap, but we can focus the dollars on those who need it most.”
The Walter family, though, may still face a nearly $200 monthly premium payment to cover both of them, $130 more than they previously paid for healthcare and prescriptions through Covered California.
“I can’t afford that, not really,” said Veronica, a pet sitter who works part-time at a school. “A giant state like this with this many people, and this many resources? You can’t just leave the people with nothing for healthcare or healthcare they can’t afford.”
California policy researchers and health advocates acknowledge the limits of a partial subsidy but say that concentrating funds on those who earn less is the most efficient way to maximize impact. People who drop coverage are often younger, healthier, and less likely to have high healthcare costs — all factors that help stabilize the insurance risk pool. Without coverage, Lee said, they’re also more likely to experience debt from medical emergencies or leave unpaid hospital bills that strain the taxpayer-funded safety net.
Cary Sanders, senior policy director at the California Pan-Ethnic Health Network, a health advocacy group, said the state’s move last year kept low-income enrollment in Covered California steady and reduced racial disparities in coverage.
“It’s working; it’s just that it’s not enough,” Sanders said. “We need the federal subsidies back.”
Still No Help for Many
When Congress passed enhanced subsidies in 2021, it capped monthly premium payments for even the highest earners at 8.5% of income. Those temporary enhancements allowed about 8 million Americans to choose robust plans with no monthly premium payment last year and helped double Obamacare enrollment to an all-time high of 24 million.
At the end of last year, 22 million of them lost that help when the GOP-led Congress blocked the extension.
The pressures on Obamacare enrollees don’t stop at premiums. Federal legislation Republicans passed last summer known as the One Big Beautiful Bill Act also shortens enrollment windows, tightens income verification requirements for subsidies, and requires enrollees who earn more than they projected to pay back the full amount.
Even if Newsom’s proposal passes, most Covered California customers won’t get state help. Nearly 1 million enrollees — 52% — earn above the $31,300-a-year individual earning cutoff.
Victoria Garzouzi was one of many middle-income retirees hit with one of the most extreme premium increases: The monthly payment for her low-level bronze plan jumped eightfold to $1,600.
To make ends meet, she came out of retirement and dipped into her savings. “I’m working to pay for my insurance,” she said. “I am an army of one.”
Despite a $6,000 deductible, her health insurance premium payment is more than the mortgage on her two-bedroom house. She’s putting off a needed cataract surgery until October, when she turns 65 and qualifies for Medicare.
While GOP leaders have not publicly weighed in on the state subsidies, some Democratic lawmakers have questioned why more help hasn’t been proposed.
Assembly member Dawn Addis, who chairs the chamber’s budget subcommittee on health, suggested Newsom could tap an additional $230 million from a fund for healthcare cost relief — money raised from a state penalty levied on those who can afford to enroll in health insurance but choose not to.
Lawmakers have previously criticized state officials for socking away much of the penalty revenue, which was supposed to go toward healthcare affordability. After California discontinued its premium subsidies thanks to increased federal assistance, the Newsom administration said the state was saving to help consumers once those temporary subsidies expired. Instead, California borrowed from the subsidy fund to cover state budget shortfalls, to the tune of $771 million. Starting this year, the subsidy fund should see an influx of cash as the state pays back the loan.
At a May legislative hearing, Joseph Donaldson, then a Department of Finance analyst, said maintaining the reserve was a prudent and financially sustainable approach.
Dylan Roby, a public health professor at the University of California-Irvine who consults for Covered California, said the focus on lower-income enrollees is deliberate. They qualify for federal subsidies that higher earners don’t, maximizing federal investment and strengthening the broader system.
“You end up with more advanced premium tax credits flowing into the state that you would have been leaving on the table,” he said.
State lawmakers have until June 15 to pass a state budget. Then, Covered California’s board would decide eligibility and benefit amounts, a decision that could come this summer, with new subsidies starting Jan. 1.
Even with the extra help, Walter and her husband worry they won’t be able to afford a potential $200 monthly premium payment. Walter said she’d likely have to rely on free clinics or ration medications.
“I take so many pills, I rattle,” she said. “That, on top of the $200? For us, it really adds up.”
A pet sitter and part-time school employee, Veronica Walter is worried she and her husband wouldn’t be able to afford monthly health insurance premiums next year even with more generous state subsidies. (Christine Mai-Duc/KFF Health News)
Are you struggling to afford your health insurance? Have you decided to forgo coverage? Click here to contact KFF Health News and share your story.
Trump Bought Tobacco Stocks and Raked In Industry Donations as FDA Eased Standards
Trump Bought Tobacco Stocks and Raked In Industry Donations as FDA Eased Standards
President Donald Trump grew his stock holdings this year to as much as $1.64 million in tobacco giant Philip Morris. (Cheng Xin/Getty Images)
President Donald Trump, who once declared he had “saved” flavored vapes, grew his stock holdings this year to as much as $1.64 million in tobacco giant Philip Morris.
He also had holdings in Altria and a third leading tobacco company, though an apparent discrepancy in his disclosures clouds the extent of his investments. In 2025, tobacco interests donated $6 million to MAGA Inc., a super PAC that supports the president, and Trump’s inauguration. And, on April 30, a week before FDA guidance that provided a critical boost to the industry, Reynolds American dropped an additional $5 million into the super PAC’s coffers.
The stock trades and political contributions occurred as the Trump administration pursued a broadly pro-tobacco agenda: Its FDA piloted a fast-track program to approve nicotine pouches. It unveiled a program to allow vapes on the market more rapidly, despite resistance from career civil servants and leadership, culminating this year in guidance waving through flavored electronic cigarettes. It cut public health employees focusing on anti-tobacco policy. And it broadened enforcement against illicit e-cigarettes, competitors to the big industry players with a financial relationship to Trump.
It amounts to the most pro-tobacco, pro-nicotine presidency in some time — a remarkable policy given the tens of millions of deaths cigarettes caused during the 20th century. Even in recent years, anti-smoking groups say a half-million Americans a year die from cigarettes. Industry advocates say the toll helps justify a shift to e-cigarettes and nicotine pouches, which they say are less harmful. However, public health advocates say these products carry their own risks, such as addiction.
Lawmakers and public health leaders have criticized the recent FDA guidance and approvals as a “lucrative payday” that ignored scientific evidence to deliver what investment analysts have described as “very positive” steps for influential tobacco companies.
The scale of the money is “unprecedented and problematic,” said Brian King, who was pushed out of the FDA’s tobacco office last April and now works as an executive at the Campaign for Tobacco-Free Kids. He fears that steering public policy toward tobacco — still addictive and harmful to health — puts Americans at risk.
“It’s a gift on a platter with a side of public health malpractice,” he said.
Email Sign-Up
Subscribe to KFF Health News' free Morning Briefing.
The White House did not comment on the president’s investments or industry donations to MAGA Inc. Spokesperson Kush Desai said, “The only guiding factor behind the Trump administration’s health policymaking is Gold Standard Science. FDA’s regulatory treatment of nicotine pouches and vapes is rooted in recent evidence that has found that these products can help adults quit smoking.”
Philip Morris disputed any connection. Company representatives “regularly attend events and forums where we share our commitment to improving public health in the United States,” spokesperson Samuel Dashiell said, “starting with providing better options to America’s 45 million legal-age nicotine consumers.”
“We do not comment on individual engagements or on the personal financial matters or disclosures of public officials,” he added.
Other tobacco companies whose stock Trump has bought and sold during his second term or that donated to groups aligned with Trump — Juul, Reynolds American, and Altria — did not respond to requests for comment.
The financial stakes are huge. Investment analysts at Goldman Sachs say the newer products, touted as safer, make more money per sale than traditional cigarettes. Philip Morris expects Zyn pouches, for example, to make eight times the gross profits of its cigarettes, Goldman Sachs analysts said in March 2025.
When he ran for his second term, Trump promoted himself as a pro-tobacco candidate, posting that he had “saved” flavored vaping and that President Joe Biden and Democratic nominee Kamala Harris “want everything banned.”
Since late 2023, MAGA Inc. has received over $20 million in funding from the industry, federal campaign records show. Trump’s inauguration garnered nearly $4 million more. His ballroom project has disclosed donations of an unknown amount from Altria and Reynolds American.
Recent Trump administration actions show he’s followed through with his campaign rhetoric. In May, the FDA released consequential guidance that allows manufacturers to market their vapes and nicotine pouches while awaiting agency approval. It also approved several vaping products. The month before, the Vapor Technology Association, which donated $1.25 million to Trump’s inauguration, told its vape-manufacturer members it had met with the White House to discuss its concerns.
By that point, Trump had gone on a stock-purchasing spree. In March he made eight separate purchases of Philip Morris or Altria stock, worth as much as $275,000, according to a disclosure form that bears Trump’s signature.
It is difficult to be precise about Trump’s tobacco investments, because the financial disclosures show only ranges of investment amounts. They also have an apparent discrepancy. In January, the president sold $500,000 to $1,000,000 in Altria stock. But that’s confusing because previous disclosures didn’t show Trump held that much equity in Altria. The White House declined to comment on the matter.
The FDA’s May guidance and approvals drew condemnation from public health leaders, who worry that the agency is allowing products with flavors especially appealing to young people. “After years of recognizing the dangers flavored e-cigarettes pose to youth, it is deeply troubling to see FDA ignore the scientific evidence and reverse course,” American Lung Association CEO Harold Wimmer said in a published statement.
“I think it’s blatantly illegal, both on its merits and also procedurally, because it was issued as a final guidance without even giving the public an opportunity to comment on it,” said Mitch Zeller, a former head of the FDA’s tobacco center.
A group of Democratic senators called the decision a “a free pass to addictive and harmful vapes” in letters to Reynolds American and Altria. It would lead to “a lucrative payday after years of unsuccessful legislative and regulatory efforts to weaken federal tobacco oversight,” they concluded.
Members of Congress are barred from insider trading, and many legislators would like to see trading of individual company stocks banned for all members. In the wake of Trump’s most recent financial disclosures, with revelations that he often traded in companies manufacturing GLP-1 drugs before his administration steered policy in a favorable direction, some members are calling for the president, too, to be barred from stock trading.
Trump’s tobacco policies have garnered favorable grades from investors. At Goldman Sachs, bankers described the May FDA guidance as “very positive” for Philip Morris and “a significant step in the FDA’s positioning toward enforcement and acceptance of nic pouch (as well as e-vapor) innovation generally.”
And Barclays analysts said the FDA’s guidance was good news for Juul, a leading vape producer. (In November, the company contributed $1 million to MAGA Inc.)
FDA resistance to speeding up approvals for these products reportedly contributed to the ouster of agency commissioner Marty Makary, who did not respond to requests for comment. According to The New York Times and The Wall Street Journal, the White House repeatedly intervened in the approval process.
“I served during the entire first Trump administration as center director, and there was never any pressure from any political appointee at FDA, at HHS, or the White House when it came to application review,” Zeller said.
But recent changes in FDA policy can be traced to the access tobacco firms have had to the White House, he said.
By and large, the Trump administration has delivered on industry priorities. Soon after the inauguration — which tobacco companies had donated heavily to — the administration withdrew a Biden-era proposal to ban menthol cigarettes. The administration has eased the path for nicotine pouches like Zyn, which were first approved under Biden. Investment analysts viewed government crackdowns on illicit e-cigarettes positively: Barclays wrote in January that “company commentary on enforcement has also been upbeat, suggesting that the tide could begin to turn in favour of the legal players in the market.”
What’s more, the Trump administration’s government layoffs have decimated public health’s tobacco control offices. The work of the Centers for Disease Control and Prevention’s office of smoking has been sharply curtailed; its flagship “Tips From Former Smokers” campaign, which seeks to persuade viewers not to smoke, has been off the air for months, King said.
“It’s not difficult to see that less dollars invested in prevention and control is going to lead to more tobacco product use and tobacco-related disease,” King said, especially given the government’s decades-long success in reducing cigarette usage.
The shift is particularly ironic given the administration’s focus — through its Make America Healthy Again slogan — on chronic disease. “Attempting to combat chronic disease without tobacco control is like attempting a triathlon without a bicycle: You are destined for failure before leaving the starting line,” King concluded.
FDA’s Greenlight of Old Chemical Offers Chance To Restore Faith in Sunscreen
FDA’s Greenlight of Old Chemical Offers Chance To Restore Faith in Sunscreen
Officials, environmental health advocates, and skin care industry groups are expressing hope that the Food and Drug Administration’s approval of a sunscreen ingredient on June 9 — after consideration for two decades, and global use for nearly as long — will help restore Americans’ wavering faith in sunscreen.
“Bemotrizinol has been used safely in Europe for decades,” Health and Human Services Secretary Robert F. Kennedy Jr. said in the announcement about the approval. “FDA’s action will increase competition and consumer confidence in sunscreen products.”
Nonprofits that advocate for health, such as the Environmental Working Group, and the skin care industry alike had lobbied for approval of the ingredient, which makes sunscreens sheerer and lighter on the skin than many available American options while blocking a wider spectrum of ultraviolet rays that can cause premature aging and skin cancer.
The newly approved sunscreen filter will allow companies to reformulate sunscreens to address consumers’ concerns, said Carl D’Ruiz, a senior manager at DSM-Firmenich, a Swiss maker of sunscreen chemicals that applied for the FDA approval. In addition to allowing companies to offer what the FDA calls safe and effective formulations, he said, the approval will allow sunscreens that are more like sought-after South Korean brands to be sold in the U.S. by autumn.
Confidence in U.S. sunscreen has faltered on two fronts: among those concerned about what’s in the sunscreens they use and those who believe sun exposure is healthy. But will the new ingredient win the trust of Make America Healthy Again skeptics and Gen Zers intentionally tanning? RFK Jr., strikingly bronzed, has helped stoke this confusion by pledging in 2024 to fight what he called the FDA’s “war on public health” and “aggressive suppression” of sunshine. Under his leadership, the FDA backed away from a plan in March to ban people under 18 from using tanning beds.
All this matters because 1 in 5 people will develop skin cancer by age 70 in the United States. It is the most common cancer in the nation, where about 3.3 million people are diagnosed each year with basal and squamous cell carcinomas.
Email Sign-Up
Subscribe to KFF Health News' free weekly newsletter, "The Week in Brief."
D’Ruiz said he thinks bemotrizinol, also known as BEMT, will change the dynamic. “People will talk more positively about sunscreens,” he said.
In the U.S., new sunscreen chemicals are regulated as over-the-counter drugs like aspirin or cough syrup rather than as cosmetics, as in Japan and the European Union. That means they face more elaborate testing and safety protocols, such as animal testing that runs afoul of EU laws, which is why the approval process for bemotrizinol took nearly two decades, D’Ruiz said.
What’s “generally recognized as safe and effective,” otherwise known as “GRASE” in FDA-speak, is at the center of the American sunscreen debate. Bemotrizinol joins zinc oxide and titanium dioxide on the FDA’s GRASE list.
That could help rebuild trust, said Alexa Friedman, an environmental epidemiologist at the Environmental Working Group, a nonprofit that researches the ingredients in consumer products.
“It has strong safety data,” Friedman said. “The documents submitted to the FDA to achieve ‘generally recognized as safe and effective’ include tests of irritation, sensitization to allergies, two-year animal studies for carcinogenicity, and reproductive health.”
The approval will also give consumers access to sunscreens that don’t leave as much of a white cast, she said, which makes some people hesitant to use mineral sunscreens such as zinc oxide and titanium dioxide.
Bemotrizinol’s approval won’t change the possibility of several chemicals with unclear safety profiles being added to sunscreens.
In 2019, the FDA said there was insufficient data to support a positive “generally recognized as safe and effective” determination for 12 commonly used sunscreen chemicals.
The concerns emerged after the FDA published a study that said some sunscreen ingredients had been found in humans’ bloodstreams. Though the industry has since phased out several of those chemicals lacking GRASE status, four are still widely used: avobenzone, homosalate, octisalate, and octinoxate.
“The European Union had recently concluded that homosalate was not safe at concentrations that they were using and recommended a very low percentage — which was effectively a ban,” Friedman said. “The U.K. also issued a safety evaluation.”
Octisalate and octinoxate have been associated with disruption of the endocrine system, and octinoxate was banned for sale in Hawai‘i due to concerns that it harms marine life and bleaches coral reefs.
Avobenzone breaks down when exposed to light, making it less effective, Friedman said, and has been associated with allergic reactions.
Mark Mitchnick, a pediatrician who invented transparent zinc oxide, which is known under the brand Z-Cote, said bemotrizinol will give chemists a new tool to make sunscreens that people will want to wear.
“It’s a good UVA block,” he said. “It gives us good flexibility. In my mind, it allows you to make really good products without using avobenzone, which I think has a lot of baggage.”
Most of the UV rays people are exposed to are UVA rays that can penetrate the middle layer of the skin and cause up to 90% of skin aging, along with a smaller amount of UVB rays, which are responsible for sunburns. Ultraviolet radiation falls on the electromagnetic spectrum between X-rays and visible light.
Mitchnick said major companies have used chemical filters because they work better on a per-pound basis compared with mineral sunscreens made with zinc oxide and titanium dioxide. “That’s why hybrids are great — you get the best of both worlds.” He said he expects companies, including his own, to release hybrid products containing bemotrizinol and zinc oxide later this year.
J. Frank Nash, a senior director and research fellow at Procter & Gamble, said skepticism about sunscreen is unfortunate because properly formulated sunscreens do an excellent job blocking solar UV, “which we know is responsible for skin cancers and aging.”
He worries the industry has contributed to the trust gap by adding unapproved UV filters, called boosters, to mineral sunscreens, to raise sun protection factor ratings, or SPF. This leads consumers to wonder what’s in the products they’re buying.
Still, in Australia, where bemotrizinol has been used in sunscreens for years, a recall scandal over ineffective products shows that even when regulators allow lauded UV filters, bad actors can taint a whole industry.
“People are not shunning sunscreen because they have stopped believing UV is dangerous,” said Joseph Mizikovsky, a director of the Australian Sunscreen Council. “They are shunning it because they have lost trust in what is in the bottle.”
He applauds the FDA’s transparency with American consumers about the lack of safety data for filters without GRASE status, and FDA’s insistence on mandatory microbial testing of products.
But he said the FDA could do more to rebuild trust in sunscreens.
“My view is the FDA should move faster to ban filters that are missing safety data, and the public should focus on physical protection — shade, clothing, hats, sunglasses — with sunscreen as the last layer, not the first.”
Anguished Parents. Doctors in Tears. Utah’s Long Measles Outbreak Takes a Toll.
Anguished Parents. Doctors in Tears. Utah’s Long Measles Outbreak Takes a Toll.
The state’s outbreak means adapting to America’s new reality, in which vaccine-preventable diseases become common again.
Kandace Hyland, a marketing director in Utah, was surprised to learn that daycare staff in the state don’t have to be vaccinated against measles, even amid an ongoing outbreak. “I’m nervous sending her to daycare every day,” she says of her baby. (Amy Maxmen/KFF Health News)
Anguished Parents. Doctors in Tears. Utah’s Long Measles Outbreak Takes a Toll.
The state’s outbreak means adapting to America’s new reality, in which vaccine-preventable diseases become common again.
SALT LAKE CITY — Ben Dowse hadn’t expected to treat measles when he became a doctor, but there he was, examining a newborn exposed to the virus in the womb. The infected mother had given birth just hours earlier. The hospital had alerted Dowse to the case before delivery, and he’d braced himself for the worst.
Dowse wore a full-body protective suit with a plastic face mask. As a pediatrician in southern Utah, he couldn’t risk getting even a mild infection, because many of his patients are babies too young for measles vaccines or children whose parents choose not to protect them with immunizations. “I went in looking like a scientist in E.T.,” he said.
Measles can cause brain damage, deafness, or death in newborns. If the baby entered the world with a measles rash and fever, Dowse was prepared to give the infant a spinal tap to assess the risk of neurological damage.
Luckily, flushed and crying, the baby looked healthy. To keep it that way, Dowse wanted to inject the baby with concentrated antibodies against the measles virus. To his surprise, the parents objected, promising to give their child “all kinds of vitamin A,” Dowse said. He begged them not to, saying, “You can’t see it on the surface, but the baby’s body is fighting the measles.” They were afraid of vaccines, so Dowse explained that antibodies were different and that they would stop measles from replicating in the infant.
“That shot is going to basically give the baby ammo to fight,” Dowse said.
The parents relented. A couple of days later, they left the hospital with a child who had narrowly skirted an infection that killed many thousands of babies a century ago. Nonetheless, Dowse said he doubted they would be returning for childhood vaccinations to protect their baby against a bevy of illnesses. Like more than a dozen Utah doctors and health officials who spoke with KFF Health News, Dowse has adjusted his expectations.
He is part of a reluctant cohort of medical professionals now on the front line of America’s regressive next chapter in health history, one in which dangerous and preventable diseases return.
“I wish that people could see what I see,” said Nathan Money, a hospital pediatrician in Utah whose eyes welled up with tears as he described children he’s treated for measles struggling to breathe. “This train is going in the wrong direction, and it can feel like a helpless situation, because we’re just not seeing the public messaging and leadership that’s needed to turn this around.”
Since measles was deemed eliminated in the U.S. a quarter century ago, public health workers have extinguished sporadic outbreaks in close-knit, undervaccinated communities with targeted methods: Isolate people with measles and quarantine their contacts to contain the virus. But as vaccination rates drop nationwide, the virus is moving beyond insulated communities, overwhelming public health departments constrained by shoestring budgets. Larger outbreaks, the kind not seen for a generation, have forced health officials into a new paradigm: They have stopped racing to “contain” infections and shifted gears into what they call “mitigation.”
Utah made that transition early this year, once the outbreak hit “a point where you no longer have control over it,” said state epidemiologist Leisha Nolen. By March, measles had been detected in every health jurisdiction in the state and in northern Arizona. More than 950 people have tested positive in the two states since the outbreak began in August, but many people with measles haven’t been tested. A genetic analysis of measles viruses suggested that the true number of cases last year could have been 6.5 times what was known.
Last year under President Donald Trump, U.S. measles cases exceeded 2,000 for the first time since 1992. Six months into 2026, the U.S. has already surpassed that threshold. Prolonged outbreaks exact a toll on children, who have spent days in hospitals for severe infections and missed weeks of school for mild ones. Adults with measles miss work. Parents delay daycare to keep their babies safe. Doctors in Utah have enacted labor-intensive protocols to keep measles from spreading in clinics. Newborns and people with weakened immune systems who have been exposed to the virus receive infusions of concentrated antibodies costing $500 to $1,000. Medical visits for measles can costmore than $33,000 per patient. Health departments spend millions trying to curb infections.
Emilie Morris, a hospital pediatrician in Utah, has cared for multiple unvaccinated children who were severely sick with measles. She’s learning how to communicate with parents who hadn’t expected the virus to cause so much harm. (Amy Maxmen/KFF Health News)
“This is like a snowball that gathers speed as it rolls downhill,” said Emilie Morris, a hospital pediatrician in Salt Lake County and Utah County. A full-throttle campaign to educate communities on the safety of vaccines and the diseases they prevent could turn the situation around, doctors and health officials said. It would require an effort similar to what the anti-vaccine movement has long done in videos, blogs, and podcasts. For example, the anti-vaccine organization that Robert F. Kennedy Jr. founded before taking the helm at the Department of Health and Human Services, Children’s Health Defense, visits vaccine-hesitant communities, produces movies, and has bought advertisements on Facebook that downplay the threat of viruses while wildly exaggerating the risk of vaccine side effects. Kennedy’s words and actions as health secretary are adding to parents’ doubt.
After the development of vaccines and antibiotics in the mid-1900s, virologist and Nobel laureate Frank Macfarlane Burnet wrote, “One can think of the middle of the twentieth century as the end of one of the most important social revolutions in history, the virtual elimination of the infectious diseases as a significant factor in social life.”
He couldn’t have imagined what was coming.
‘Year of Sickness’
A view of St. George, a city in southwest Utah that’s been hit hard by an ongoing measles outbreak that started in August. Nearly 40% of the state’s cases have occurred in the region. (Amy Maxmen/KFF Health News)
In communities nestled among the red sandstone cliffs and riparian forests of southern Utah, measles took hold last summer. At the main school in Hildale, a town along the Arizona border, just 30% of kindergartners are considered adequately immunized by Utah’s health department, meaning they’ve gotten recommended vaccines against measles, tetanus, polio, and more. Exemptions from childhood vaccine requirements are easily acquired in the state: Parents need only claim personal, religious, or medical reasons.
Many people in Hildale and the surrounding towns are connected to the Fundamentalist Church of Jesus Christ of Latter-Day Saints, a sect that has been leery of the government since a police raid in 1953 separated polygamous parents from their children. Shirlee Draper, a southern Utah resident who grew up in the faith, said they became ever more isolated in the early 2000s under the leadership of Warren Jeffs. Before he was sentenced to life in prison for sexual assault against minors, Jeffs instructed his followers to withdraw from public schools and mainstream medicine.
“Growing up, we all got our vaccines,” said Draper, who left the group during Jeffs’ reign. “It wasn’t until Warren Jeffs came along that there started to be more and more resistance.”
After Jeffs went to prison, many people left the faith but remained concerned about vaccines because of online misinformation, such as claims that the shots are toxic. Today a small shop in Hildale sells mouth sprays and oral drops professing to detoxify vaccines. Water, glycerin, and “whole grain alcohol” are listed as ingredients in one called Vxx-Dtx.
A mother who KFF Health News agreed not to name, because she fears stigmatization, said she considered getting her kids vaccinated when schools in southwest Utah started seeing measles cases last summer. She had split from the fundamentalist group but still worried about vaccines giving her children autism or other complications. Largestudiespublished in top-tier scientific journals have refuted a link between vaccines and autism, but the anti-vaccine movement has kept the notion alive.
Then the woman’s son told her that his classmate had a rash and spit on him, she said. A few days later, he fell ill with a fever, followed by vomiting, diarrhea, and a head-to-toe rash.
“He felt downright sick for 10 to 14 days,” the woman said. “It was hard to see the end of the tunnel.”
Then her daughters came down with measles. She had a fleeting case, too, even though she had been vaccinated as a child. Breakthrough infections tend to be mild and are relatively rare. Only 4% of 4,300-plus U.S. cases reported this year and last have been among people who’ve had two doses of the measles, mumps, and rubella vaccine.
By the time the family recovered, the son had missed nearly three weeks of school, the daughters a month, and the mother had postponed an important family gathering because she didn’t want to spread infections. “I just got my youngest’s missed-school report and it’s super high,” she said. “This is the year of sickness.”
The Southwest Utah Public Health Department stocks vaccines against measles, whooping cough, tetanus, hepatitis B, and other diseases. (Amy Maxmen/KFF Health News)
The woman said she regretted not getting her kids vaccinated when the outbreak started. She said she knows about 30 people who have fallen sick with the measles. Except for a few who needed medical care, they haven’t been tested. “I bet there’s been thousands of cases,” she said.
Measles doesn’t have a cure. She and others have tried to ease symptoms with cod liver oil, vitamin C, zinc, and “essential oils,” plant extracts long used in folk medicine that have become a lucrative industry in Utah. People in southwest Utah are trying a lot of things: One resident sells homemade lotion on Facebook, writing, “Breastmilk & Honey has been a life saver for the measles rash.”
Email Sign-Up
Subscribe to KFF Health News' free weekly newsletter, "The Week in Brief."
Beyond Containment
The outbreak may have started among a fundamentalist community, but it’s spread far beyond because Utah’s vaccination rates have dropped steadily since the covid pandemic. Fewer than 80% of kindergartners were adequately immunized in the 2024-25 school year in southwest Utah, with only 87% adequately immunized in the state as a whole — far below the 95% threshold required for herd immunity.
Several Utahns told KFF Health News that “alternative health” or “wellness” drives the trend, rather than religion. The state has a thriving supplement industry, worth $6.1 billion in 2023, aided by deregulatory policies supported by the late Utah senator Orrin Hatch and a high concentration of people who earn income from multilevel marketing. These networks of people sell supplements, essential oils, peptides, and other alternative therapies on social media, YouTube, and podcasts, according to scholarly articles and industry analyses.
Alternative health isn’t necessarily anti-vaccine, but many people who sell unconventional remedies online and in podcasts deride vaccines and mainstream medicine.
“People are suspicious, and it’s well founded,” Draper said. She described dismissive doctors, exorbitant medical bills, hospital systems that put profitsover care, and pharmaceutical companies that drove opioid addiction. Communities already wary of government authorities are poised to interpret failings in American healthcare as signs that medical authorities aren’t to be trusted, either, she said.
“Across America, we have entire populations who find safety in clinging to whatever confirms their deeply held beliefs,” she said.
A mistrustful disposition gave way to covid conspiracy theories in 2020 and 2021. In southwest Utah, for example, a pickup truck tricked out with digital billboards showed up to covid vaccination sites to advertise Plandemic, a 26-minute viral video rife with conspiratorial claims, including that masks “activate” the coronavirus and that global elites planned covid-19 to control the population. Misinformation added fuel to anger about public health rules, and there was political backlash under the umbrella of a largely Republican “medical freedom” movement. Utah enacted laws reining in public health, including one that eases exemptions to childhood vaccinations and another that prohibits most employers from requiring vaccines.
In the wake of the covid backlash, health officials tread lightly. Rather than enforce containment measures, “we give our advice and focus on personal responsibility,” said David Heaton, public information officer at the Southwest Utah Public Health Department.
Utah state epidemiologist Leisha Nolen says that with a larger budget she would invest in connecting with communities. “We have a scientific solution,” she says about measles, “but we need a societal solution, too.” (Amy Maxmen/KFF Health News)
One of the most contagious diseases in the world, measles spreads with astonishing speed among the unvaccinated. One meticulous study of a New York school outbreak in 1974 found that a second-grader with measles infected 28 other students in 14 classrooms because measles can spread through ventilation systems.
As cases doubled then quadrupled in southern Utah, the regional health department couldn’t keep up with calling the contacts of everyone infected. It shifted its efforts to announcements guiding the public at large. For example, it asks people to call before showing up to clinics with measles symptoms. Still, patients in plenty of hospitals have been exposed. For example, when parents brought a sick, unvaccinated child to a large pediatric hospital in Utah in September, they shared the space with 11 infants too young to be vaccinated. Doctors rushed to give the babies infusions of antibodies and they remained healthy, according to a recent report.
On the radio and in posts on social media, Heaton warns that measles is spreading and that vaccines are the best defense. “If you’re not immunized and you’re anywhere in public,” Heaton said, “you’re fair game for this virus.”
The department doesn’t have the capacity to talk with people directly in the five counties it serves. For a few years, it leaned on community health workers who went to churches, town halls, and other gathering places, listening to people’s concerns and telling them what the science said about covid, vaccines, and other matters of public health. But these workers were laid off early last year, after the Trump administration clawed back more than $12 billion in federal public health grants to states.
“We were starting to get a little bit of traction,” Heaton said of the community workers. “And then we lost all of our team.”
The department offers free measles vaccines to children, but uptake is slow. Nursing director Mindy Bundy said that when she started the job 20 years ago, demand was so high that she would give parents tickets while they waited, as if they were crowding around a deli counter.
“Now even in an outbreak,” she said, “we aren’t seeing a huge increase of people wanting vaccination.”
Anna Fajardo, a public health nurse, offers vaccines at a school registration event in Milford, in southwest Utah. A few mothers trickled in to get their children immunized or to find out their child’s vaccination status. (Amy Maxmen/KFF Health News)
As officials tried to do the best they could, the outbreak spread north, hopping from one undervaccinated community to the next. When health officials in Utah County spoke with people who had tested positive, they often had no connection to other known cases. “Pretty quickly, we started to lose the links,” said Michael Leman, the county health department’s nursing director. Contact tracing, the cornerstone of containment, was failing.
Every week, the state health department posted a growing list of locations on its website — a Trader Joe’s, a Mormon temple, an aquarium, preschools — that people had visited while contagious. But many people who tested positive hadn’t been to those places, Leman said. “They could have gotten it at Walmart. They could have gotten it walking through a mall,” he said. “I mean, just anywhere in the public they could have been exposed.”
In February, high school students throughout Utah tested positive after a state wrestling tournament at Utah Valley University in Orem. A dashboard monitoring measles viruses in wastewater lit up with notifications around the state. “Wrestling really feels like our turning point,” said Nicholas Rupp, communications director at the Salt Lake County Health Department.
The new Lindon Utah Temple, belonging to the Church of Jesus Christ of Latter-Day Saints, was one of many locations listed as a potential measles exposure site in April by the Utah Department of Health and Human Services. (Amy Maxmen/KFF Health News)
A Trader Joe’s in Orem, Utah, was also listed as a potential measles exposure site that month. (Amy Maxmen/KFF Health News)
A science building at the University of Utah in Salt Lake City was also among the potential exposure sites listed in April. (Amy Maxmen/KFF Health News)
Many measles cases traced back to a high school wrestling tournament at Utah Valley University in Orem in February. (Amy Maxmen/KFF Health News)
Salt Lake County’s shift from containment to mitigation meant prioritizing high-risk situations and relaxing control everywhere else. When a student has a confirmed case, for example, health officials meet with the school nurse to figure out which kids are most vulnerable. Unvaccinated children in the same classroom as someone infected are asked to stay home for 21 days, but those in other classrooms might not be, said Melanie Crossland, an epidemiologist at the Salt Lake health department. Some schools with high vaccination rates have opted to monitor student temperatures daily instead of requesting quarantines. One school created a separate space for the unvaccinated.
Crossland said such bespoke strategies entail a “huge” amount of effort but have staved off blowback that deflated her during covid.
“We give everything when we’re here,” she said, “but the days of killing ourselves, when legislatively no one is going to give us any help, are done.”
Daycare Dilemma
The outbreak has lasted so long that some children who have recovered from measles have since been hospitalized for what should be mild illnesses from common bugs, said Kerri Smith, a hospital pediatrician in southwest Utah. Measles can erase the immune system’s memory, impairing a body’s ability to fight other viruses. “It’s making children very susceptible to getting sick again,” Smith said.
Her eyes were bloodshot, and she looked drained from a week of long shifts. Since the outbreak began, she’s treated more than a dozen babies and children severely sick from measles.
“They’re usually admitted to the hospital with measles pneumonia, so they’re struggling to breathe, pulling for air below their ribs,” she said. “High fevers, 104 to 105, absolutely miserable, extremely fatigued, really dehydrated with sunken eyes.” Most children fully recover from measles, but a fraction develop permanent hearing loss, a small percentage die, and in rare cases, measles kills a person years after the infection.
No one has died so far in Utah’s outbreak. And barring that tragic outcome, Smith and other doctors said, some parents fail to grasp the gravity of measles, even as their own children have tubes inserted into their small nostrils to deliver oxygen. Despite repeated warnings, doctors said, some unvaccinated family members of patients — who could be contagious — walk around the hospital while visiting their loved one. This means the waiting room, the elevator, the cafeteria, and other places need to be shut down for cleaning, and vulnerable people alerted.
“People don’t realize how easily this spreads,” Smith said.
Morris, the pediatrician working in two counties, recalled a conversation with a nonchalant father who didn’t seem to understand the need for quarantine. “I know this is an inconvenience to you,” she said. “It’s also a huge inconvenience to the parent who has an infant who could be severely impacted by this disease.”
On top of feeling depleted, doctors with young children said they are anxious. Emily Chin, a physician in Salt Lake County, worries she’ll bring measles home to her newborn. One evening, she sat in her garage after caring for a child with a rash. The patient’s measles test was still being processed, so Chin isolated herself in a room for the night, wearing an N95 mask instead of holding her infant.
Emily Chin’s 4-month-old, sleeping here at home, is too young to be vaccinated, and Chin, a doctor in Salt Lake County, Utah, worries that she might acquire measles at work and pass it to him. (Amy Maxmen/KFF Health News)
Like many mothers in Utah, Chin plans to give her baby an early dose of the measles vaccine at 6 months old because of the outbreak, in addition to two doses at ages 1 and 4. Several mothers said they avoid travel and public places because they fear their babies could be infected. Some are delaying daycare. Others, like Kandace Hyland, a marketing director in Salt Lake County, don’t have that option.
Hyland was shocked when her daycare told her that it didn’t track the vaccine status of staff, even amid the outbreak. In March, she posted an online petition calling for the state to require daycare staff to be vaccinated against the measles when the virus is spreading. Even if daycare staff file for vaccine exemptions, she said, parents could at least find out what portion of their babies’ caretakers pose a life-threatening risk.
Hyland sent her idea to the state health department. Nolen, the state epidemiologist, said she agreed with the concern, and was “talking with the division of licensing about the issue,” in an email shared with KFF Health News. Hyland also wrote the Division of Licensing and Background Checks. In an email, its director, Shannon Thoman-Black, replied that the division does “not have the legislative authority to implement a mandate.”
“They always talk about parents’ choice,” Hyland said. “But I don’t feel like I have a really good ‘parents’ choice’ right now.”
Measles’ Comeback
The U.S. will almost certainly lose its measles elimination status this year or next, but it could be regained if political leadership backed nationwide campaigns to boost confidence in vaccines, said Demetre Daskalakis, a former director of the Centers for Disease Control and Prevention’s national immunization center and now the chief medical officer at the Callen-Lorde community health center in New York.
“Under Secretary Kennedy’s leadership, that’s unlikely to happen,” he said. “We’re going back to a pre-vaccine era.”
A sign outside a hospital in southwest Utah warns people who haven’t been vaccinated against measles to wait outside if they have a fever and other symptoms, such as coughing or a runny nose. Vulnerable people, including infants too young for vaccination, have been exposed to measles at hospitals and clinics. (Amy Maxmen/KFF Health News)
HHS spokesperson Emily Hilliard defended the secretary and his agency in an email, writing that the CDC has “surged resources” to contain measles outbreaks. “The CDC, HHS principles and the Secretary have been vocal that the MMR vaccine is the best way to protect yourself against measles,” she said.
Kennedy’s words and actions suggest otherwise. He’s said that the measles vaccine leads to “deaths every year,” which is not true. He continuestotout a potential link between autism and vaccines, no matter how many studiesconclude there is none. And he oversaw abrupt changes to the recommended childhood vaccine schedule, a move medical societies called dangerous and not backed by science. A federal judge blocked those changes in March, but Trump recently issued an executive order to reexamine the schedule.
“It’s been confusing for the public,” said Dorothy Adams, executive director of the Salt Lake County Health Department.
In May, Kennedy met with Republican Utah Gov. Spencer Cox, who has said little about the state’s ongoing outbreak. Kennedy praised Utah’s action on Make America Healthy Again priorities, such as banning fluoride in public drinking water and easing restrictions on raw milk sales, according to Salt Lake City’s Deseret News. Cox declined to comment for this article.
Meanwhile, the chronically depleted U.S. public health system has been further weakened by the Trump administration’s cuts and delays to public health grants.
“If you’re in the thick of it and you don’t know if you will be reimbursed, you adjust your response,” said Angela Dunn, a doctor and former Utah state epidemiologist. “This outbreak is a perfect storm of disinformation, trauma from the covid pandemic, and the drop in funding.”
Measles isn’t the only preventable malady making a comeback. As children played nearby in a sun-speckled park in Salt Lake City, Morris talked about a baby in the intensive care unit who was bleeding uncontrollably after a fall. The baby’s parents had refused an injection of vitamin K that helps blood clot in newborns. As they fretted over their infant, Morris said, she felt awful for them and regretted not being able to overcome mistrust in basic, lifesaving interventions. She had the same swirl of emotions when an unvaccinated toddler in her care recently died of whooping cough.
“I was one of the only people in the room with the nurse when the child coded,” she said with tears in her eyes. “You think, ‘I wish this child was vaccinated,’ but it’s hard because I also see how much grief these parents are holding.”
Looming Medicaid Cuts Supercharge California’s Latest Labor-Industry Fight
Looming Medicaid Cuts Supercharge California’s Latest Labor-Industry Fight
The looming impact of federal Medicaid cuts has reignited a long-simmering, costly battle between California’s medical industry and one of its largest health worker unions.
SEIU-United Healthcare Workers West, with approximately 120,000 members, has put forward two ballot initiatives to cap the pay of medical executives and require community clinics to spend the vast bulk of their revenues on patient care.
The California Hospital Association has responded with its own ballot proposal that would make it tougher for unions to spend money on political initiatives in the future. It would require approval by a union’s rank-and-file membership for any spending of $1 million or more on statewide measures, or $100,000 or more on local ones.
The competing measures, which have drawn enough verified signatures to qualify for the November ballot, come at a time when the rising cost of healthcare is emerging as a top voter concern.
The Service Employees International Union affiliate has seized upon affordability angst to resurrect a proposal for a cap on healthcare executive compensation, which it has failed to achieve multiple times before. The proposed measure garnered more than 1 million petition signatures.
“This initiative reflects the serious crisis we face and that affordability is a real thing,” said Vikas Saini, president of the Lown Institute, a Massachusetts-based healthcare think tank. “I think it also reflects grassroots anger and a desire to do something.”
Email Sign-Up
Subscribe to KFF Health News' free weekly newsletter, "The Week in Brief."
Mikey Vaughn, a certified nursing assistant at Cedars-Sinai Medical Center, said that the Los Angeles hospital, despite its reputation as the go-to place for the rich and famous, often lacks supplies and staffing levels that he and his colleagues need to do their jobs effectively and without undue stress.
“The executive pay initiative would, I hope, be used to hire staff and to actually provide better resources for our patients,” said Vaughn, a member of SEIU-UHW’s executive board and political committee.
Thomas Priselac, then-president and CEO of Cedars-Sinai Medical Center, made $8.8 million in fiscal year 2024, according to the organization’s most recent available federal tax filing. Kaiser Permanente’s CEO, Gregory Adams, made nearly $13 million in 2024. Warner Thomas, head of Sutter Health, made just under $12 million.
Cedars-Sinai spokesperson Duke Helfand said if the measure passed, the hospital would be unable to recruit and retain physicians, nurses, and specialists, dramatically impairing its ability to provide healthcare.
“Such a scenario would be disastrous not only for Cedars-Sinai but for hospitals across Los Angeles and California,” Helfand said.
The union wants to cap compensation at $450,000 a year for senior hospital and medical group executives, as well as other administrative and managerial staff. However, the initiative does not stipulate how dollars diverted from payroll must be spent.
Carmela Coyle, CEO of the hospital association, called the measure a cynical political ploy. “It’s bad policy and it’s going to have bad consequences across California,” she said.
Glenn Melnick, a healthcare economist at the University of Southern California, said that even if the initiative were fully implemented and pay cuts enacted, he doubts it would reduce the cost of healthcare for patients.
SEIU-UHW does not have an estimate of the total amount the initiative would claw back from pay packages that exceed the limit.
Opponents of the initiative note that it doesn’t target only executive pay but would affect medical practitioners who are also managers. That could include chief medical officers and chief nursing officers, as well as heads of surgery, emergency rooms, oncology, obstetrics, cardiology, and other specialties, they say.
It would be up to each hospital, health system, and physician group to report which staff members exceed the cap and by how much.
Ultimately, who is subject to the pay cap “probably will have to be battled out in court,” said the hospital association’s Coyle. “That’s why we are throwing everything we can at it.”
The second SEIU-UHW ballot initiative, on community clinics, is already in court. The California Primary Care Association, which represents clinics, filed a federal lawsuit in April seeking to invalidate it before it reaches the November ballot.
The proposed measure would require federally designated community clinics to spend at least 90% of their revenues on activities directly related to their mission of providing care for low-income populations. If it were to pass, over 90% of those clinic organizations would be on the hook for penalties totaling $1.7 billion in the first year alone and “would face similarly crippling penalties every year,” according to a report commissioned by the primary care association and conducted by the Berkeley Research Group, an international consulting company.
Louise McCarthy, president and CEO of the Community Clinic Association of Los Angeles County, said many pivotal services the clinics provide — translation and transportation, for example — would likely not be counted toward the spending requirement.
“They are targeting a group of what they see as employers and we see as the safety net,” she said.
The lawsuit cites the harm to clinics and claims the proposed spending requirement would interfere with federal authority.
Renée Saldaña, a spokesperson for SEIU-UHW, characterized the lawsuit against the initiative as “a really desperate attempt by the clinic industry to try and avoid accountability.”
SEIU-UHW, proud of its political activism, is also behind a controversial billionaire tax proposal that would impose a one-time 5% levy on California residents with fortunes over $1 billion to backfill the funding gap created by federal cuts coming down the pike under Republicans’ One Big Beautiful Bill Act. The law, passed last July and signed by President Donald Trump, is projected to squeeze over $900 billion from the Medicaid health coverage program for low-income people by 2034, including as much as $30 billion annually in California.
The hospital association, the community clinic group, and the California Medical Association, which represents physicians, oppose the wealth tax proposal. But Saldaña said all three of the union’s ballot proposals tie into an overarching strategy to counter the widening healthcare disparities caused by the federal law. Referring to the proposed pay cap, she said, “We believe the primary concern of healthcare providers, including executives, should be to serve the community, heal patients, and not be in healthcare just to enrich themselves.”
Over the years, the union has submitted dozens of local and statewide ballot initiatives, including ones to cap the pay of hospital executives, regulate dialysis clinics, and raise the minimum wage of healthcare workers.
The hospital association calculates that SEIU-UHW has spent nearly $125 million on local and statewide initiatives since 2012. But healthcare industry groups have spent far more opposing them. The hospital association data shows that the union spent nearly $36 million on three ballot proposals to regulate the dialysis industry, but dialysis companies poured in $302 million to defeat them, according to state campaign finance records.
The union’s ongoing political efforts “threaten patient access to quality health care,” according to the hospital association’s ballot initiative, which could limit how much unions spend on future ballot measures.
Saldaña hinted at a possible lawsuit should that measure pass, saying that “we don’t see the legal viability” of it. The proposal, she said, is an attempt “to silence the front-line healthcare workers.”
Ultimately, a ballot initiative won’t cure the ills that plague healthcare in the United States, said the Lown Institute’s Saini. What’s needed, he said, is “an evaluation and reimagination of healthcare.”